


These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Table of Contents
Clinical Application of Neuromuscular Techniques: Quadratus Lumborum
Assessment of Shortness in Quadratus Lumborum (Figure 4.21)
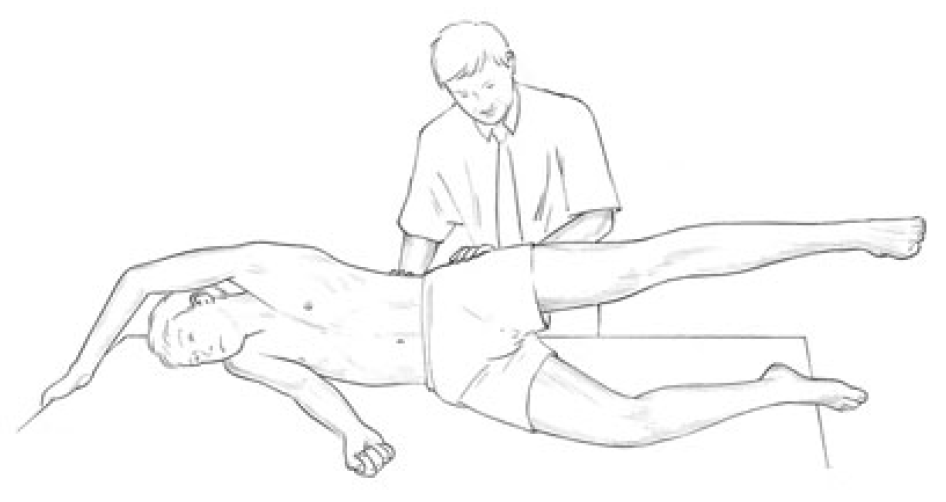
Figure 4.21 Palpation assessment for quadratus lumborum overactivity. The muscle is palpated, as is gluteus medius, during abduction of the leg. The correct firing sequence should be gluteus, followed at around 25° elevation by quadratus. If there is an immediate ‘grabbing’ action by quadratus it indicates overactivity, and therefore stress, so shortness can be assumed (see details of similar functional assessments in Ch. 5).
Review Lewit’s functional palpation test described under the heading assessment and treatment of tensor fascia lata.
When the leg of the side-lying patient is abducted, and the practitioner’s palpating hand senses that quadratus becomes involved in this process before the leg has reached at least 25° of elevation, then it is clear that quadratus is overactive. If it has been overactive for any length of time then it is almost certainly hypertonic and short, and a need for MET can be assumed.
Quadratus lumborum test (a) (See also Fig. 5.11A, B.) The patient is side-lying and is asked to take the upper arm over the head to grasp the top edge of the table, ‘opening out’ the lumbar area. The practitioner stands facing the back of the patient, and has easy access for palpation of quadratus lumborum’s lateral border – a major trigger point site (Travell & Simons 1992) – with the cephalad hand.
Activity of quadratus is tested (palpated for) with the cephalad hand as the leg is abducted, while also palpating gluteus medius with the caudad hand. If the muscles act simultaneously, or if quadratus fires first, then it is stressed, probably short, and will benefit from stretching.
Quadratus lumborum test (b) The patient stands, back towards crouching practitioner. Any leg length disparity (based on pelvic crest height) is equalised by using a book or pad under the short leg side heel. With the patient’s feet shoulder-width apart, a pure sidebending is requested, so that the patient runs a hand down the lateral thigh/calf. (Normal level of sidebending excursion allows the fingertips to reach to just below the knee.) (See Fig. 3.2A, B, C.)
The side to which the fingertips travel furthest is assessed. If sidebending to one side is limited then quadratus on the opposite side is probably short. Combined evidence from palpation (test a) and this sidebending test indicate whether or not it is necessary to treat quadratus.
Box 4.8 Notes on Quadratus Lumborum
- Norris (2000) describes the divided roles in which quadratus is involved: The quadratus lumborum has been shown to be significant as a stabiliser in lumbar spine movements (McGill et al 1996) while tightening has also been described (Janda 1983). It seems likely that the muscle may act functionally differently in its medial and lateral portions, with the medial portion being more active as a stabiliser of the lumbar spine, and the lateral more active as a mobiliser [see stabiliser/mobiliser discussion Ch. 2]. Such subdivision is seen in a number of other muscles for example the gluteus medius where the posterior fibres are more posturally involved (Jull 1994) the internal oblique where the posterior fibres attaching to the lateral raphe are considered stabilisers (Bergmark 1989) the external oblique where the lateral fibres work during flexion in parallel with the rectus abdominis (Kendall et al 1993).
- Janda (1983) observes that, when the patient is sidebending (as in method (b)) ‘when the lumbar spine appears straight, with compensatory motion occurring only from the thoracolumbar region upwards, tightness of quadratus lumborum may be suspected’. This ‘whole lumbar spine’ involvement differs from a segmental restriction which would probably involve only a part of the lumbar spine.
- Quadratus fibres merge with the diaphragm (as do those of psoas), which makes involvement in respiratory dysfunction a possibility since it plays a role in exhalation, both via this merging and by its attachment to the 12th rib.
- Shortness of quadratus, or the presence of trigger points, can result in pain in the lower ribs and along the iliac crest if the lateral fibres are affected. Shortness of the medial fibres, or the presence of trigger points, can produce pain in the sacroiliac joint and the buttock.
- Bilateral contraction produces extension and unilateral contraction produces extension and sidebending to the same side.
- The important transition region, the lumbodorsal junction (LDJ), is the only one in the spine in which two mobile structures meet, and dysfunction results in alteration of the quality of motion between these structures (upper and lower trunk/dorsal and lumbar spines). In dysfunction there is often a degree of spasm or tightness in the muscles which stabilise the region, notably: psoas and erector spinae of the thoracolumbar region, as well as quadratus lumborum and rectus abdominis.
- Symptomatic differential diagnosis of muscle involvement at the LDJ is possible as follows: psoas involvement usually triggers abdominal pain if severe and produces flexion of the hip and the typical antalgesic posture of lumbago; erector spinae involvement produces low back pain at its caudad end of attachment and interscapular pain at its thoracic attachment (as far up as the mid-thoracic level); quadratus lumborum involvement causes lumbar pain and pain at the attachment of the iliac crest and lower ribs; and rectus abdominis contraction may mimic abdominal pain and result in pain at the attachments at the pubic symphysis and the xiphoid process, as well as forwardbending of the trunk and restricted ability to extend the spine.
There is seldom pain at the site of the lesion in LDJ dysfunction. Lewit (1992) points out that even if a number of these muscles are implicated, it is seldom necessary, using PIR methods, to treat them all since, as the muscles most involved (discovered by tests for shortness, overactivity, sensitivity and direct palpation) are stretched and normalised, so will others begin automatically to normalise.
MET for Shortness in Quadratus Lumborum (‘banana’)
Quadratus lumborum MET method (a) (Fig. 4.22) The patient lies supine with the feet crossed (the side to be treated crossed under the non-treated side leg) at the ankle. The patient is arranged in a light sidebend, away from the side to be treated, so that the pelvis is towards that side, and the feet and head away from that side (‘banana shaped’). As this sidebend is being achieved the affected quadratus can be palpated for bind so that the barrier is correctly identified.

Figure 4.22 MET treatment of quadratus lumborum utilising ‘banana’ position.
The patient’s heels are placed just off the side of the table, anchoring the lower extremities and pelvis. The patient places the arm of the side to be treated behind her neck as the practitioner, standing on the side opposite that to be treated, slides his cephalad hand under the patient’s shoulders to grasp the treated side axilla. The patient grasps the practitioner’s cephalad arm at the elbow, with the treated side hand, making the contact more secure.
The patient’s treated side elbow should, at this stage, be pointing superiorly. The practitioner’s caudad hand is placed firmly but carefully on the anterior superior iliac spine, on the side to be treated. The patient is instructed to very lightly sidebend towards the treated side. This should produce an isometric contraction in quadratus lumborum on the side to be treated.
After 7 seconds the patient is asked to relax completely, and then to sidebend towards the nontreated side, as the practitioner simultaneously transfers his bodyweight from the cephalad leg to the caudad leg and leans backwards slightly, in order to sidebend the patient. This effectively stretches quadratus lumborum. The stretch is held for 15–20 seconds, allowing a lengthening of shortened musculature in the region. Repeat as necessary.
Quadratus lumborum MET method (b) (Fig 4.23) The practitioner stands behind the side-lying patient, at waist level. The patient has the uppermost arm extended over the head to firmly grasp the top end of the table and, on an inhalation, abducts the uppermost leg until the practitioner palpates strong quadratus activity (elevation of around 30° usually).
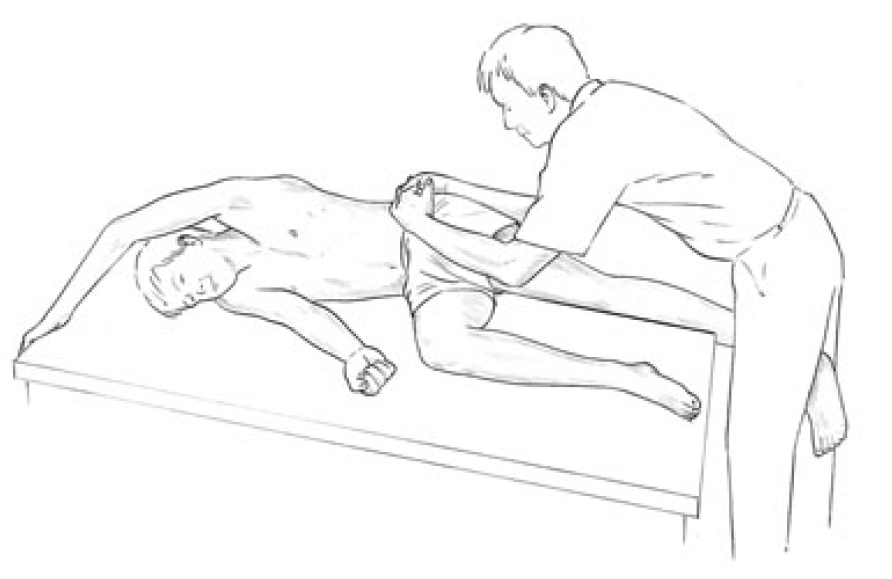
Figure 4.23 MET treatment of quadratus lumborum. Note that it is important after the isometric contraction (sustained raised/abducted leg) that the muscle be eased into stretch, avoiding any defensive or protective resistance which sudden movement might produce. For this reason, body weight rather than arm strength should be used to apply traction.
The patient holds the leg (and, if appropriate, the breath, see Box 4.2) isometrically in this manner, allowing gravity to provide resistance. After the 10-second (or so) contraction, the patient allows the leg to hang slightly behind him over the back of the table. The practitioner straddles this and, cradling the pelvis with both hands (fingers interlocked over crest of pelvis), leans back to take out all slack and to ‘ease the pelvis away from the lower ribs’ during an exhalation.
The stretch should be held for between 10 and 30 seconds. (The method will only be successful if the patient is grasping the top edge of the table, so providing a fixed point from which the practitioner can induce stretch.)
Contraction followed by stretch is repeated once or twice more with raised leg in front of, and once or twice with raised leg behind the trunk in order to activate different fibres. The direction of stretch should be varied so that it is always in the same direction as the long axis of the abducted leg. This calls for the practitioner changing from the back to the front of the table for the best results. When the leg hangs to the back of the trunk the long fibres of the muscle are mainly affected; and when the leg hangs forward of the body the diagonal fibres are mainly involved.
Quadratus lumborum MET method (c) Gravity-induced postisometric relaxation of quadratus lumborum – self-treatment (See Fig. 3.2A–C and captions) The patient stands, legs apart, bending sideways. The patient inhales and slightly raises the trunk (a few centimetres) at the same time as looking (with the eyes only) away from the side to which side-flexion is taking place. On exhalation, the sidebend is allowed to slowly go further to its elastic limit, while the patient looks towards the floor, in the direction of the side-flexion. (Care is needed that very little, if any, forward or backward bending is taking place at this time.) This sequence is repeated a number of times.
Eye positions influence the tendency to flex and sidebend (eyes look down) and extend (eyes look up) (Lewit 1999). Gravity-induced stretches of this sort require holding the stretch position for at least as long as the contraction, and ideally longer. More repetitions may be needed with a large muscle such as quadratus, and home stretches should be advised several times daily. Quadratus lumborum MET method (d) The side-lying treatment of latissimus dorsi described below also provides an effective quadratus stretch when the stabilising hand rests on the pelvic crest (see Fig. 4.29).
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez

Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.

WELLNESS TOPIC: EXTRA EXTRA: Managing Workplace Stress
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Comments are closed.