

[et_pb_section bb_built=”1″][et_pb_row][et_pb_column type=”4_4″][et_pb_text _builder_version=”3.0.95″ background_layout=”light”]
Table of Contents
THE HISTORY OF FIBROMYALGIA SYNDROME
![]() Fibromyalgia syndrome (FMS) is a relatively new diagnostic entity that surfaced in the rheumatology literature in the late 20th century. Certain patients experienced widespread aches and pains not confined to any specific muscle or joint. At first it was
Fibromyalgia syndrome (FMS) is a relatively new diagnostic entity that surfaced in the rheumatology literature in the late 20th century. Certain patients experienced widespread aches and pains not confined to any specific muscle or joint. At first it was
assumed that these patients had early signs of rheumatoid arthritis, lupus, ankylosing spondylitis, or some other systemic arthritic
processes. However, for this particular type of patient, serum laboratory testing, such as sedimentation rate, HBLA, and rheumatoid factor, showed negative results. Rheumatologists began to talk among themselves about this interesting type of patient who appeared to have a musculoskeletal disorder but, at the same time, did not have any physical examination or laboratory findings suggestive of any specific diagnosis. The only positive physical finding was a characteristic lowered pain threshold over various soft tissues on digital pressure, which were termed tender points (TePs). There was also the curious finding that most of these patients also had an associated sleep disorder that seemed to correlate with the number of TePs.1,2
In 1989, a rheumatology consensus conference was held in Minneapolis, at which time this issue was discussed in great detail. This meeting resulted in publication the follow- ing year of what has become known as the 1990 American College of Rheumatology (ACR) criteria for the classification of fibromyalgia syndrome.3 Essentially, this was the birth of FMS as a new medical term. Although the 1990 ACR criteria were meant to be merely “classification criteria” for research purposes, they quickly filled the void and became used as “diagnostic criteria” by physicians eager to have some established criteria for making the diagnosis of FMS. Essentially, the ACR standard consists of just 2 criteria: (1) chronic, widespread pain (pain that is present on both sides of the body, above and below the waist, and in the axial skeleton) that has been present for more than 3 months, and (2) pain elicited by palpation of TePs. The presence of “pain” was determined by use of an algometer during digital examination, when less than 4 kg of pressure over a TeP evoked a painful response. For a diagnosis of FMS, the required finding was pain induced on palpation of a mini- mum of 11 of 18 predetermined TeP sites.
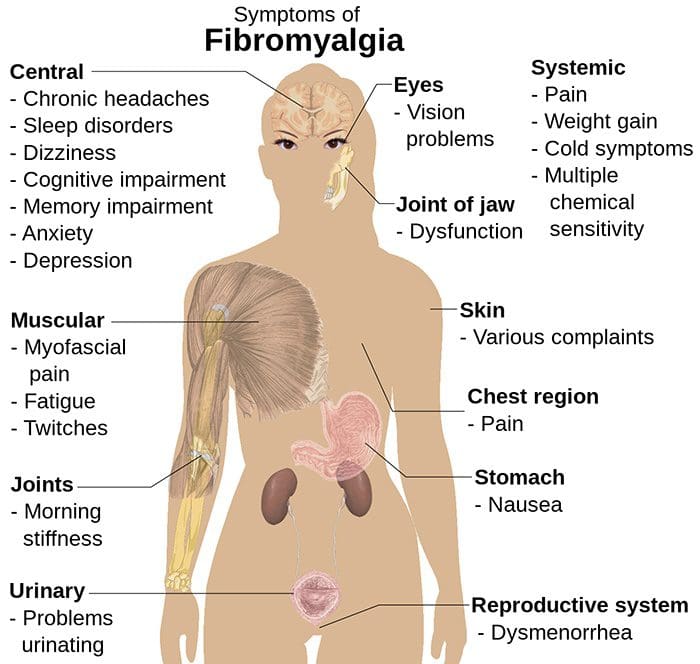
By the early 1990s, numerous authors were reporting many other symptoms associated with FMS in addition to the well-known sleep disorder. These symptoms included fatigue, irritable bowel, headache, cold sensitivity, atypical patterns of paresthesia, exercise intolerance, anxiety, depression, irritable bladder, dysmenorrhea, bruxism, and other symptoms suggestive of increased sympathetic nervous system activity. There was an emerging concept that FMS had a strong association with anxiety and depression, as well as a characteristic sleep disorder. In 1992, another FMS consensus conference was held in Copenhagen, which resulted in publication of what is known as the Copenhagen Declaration.4 The concluding remarks of the Copenhagen Declaration were as follows: “Fibromyalgia syndrome is a painful, non-articular condition predominantly involving muscles; it is the commonest cause of chronic, widespread musculoskeletal pain. It is typically associated with persistent fatigue, non-refreshing sleep and generalized stiffness. Women are affected some 10 to 20 times more often than men. FMS is often part of a wider syndrome encompassing headaches, irritable bowel syndrome, irritable bladder, dysmenorrhea, cold sensitivity, Raynaud’s phenomenon, restless legs, atypical patterns of numbness and tingling, exercise intolerance, and complaints of weakness. A varying proportion (20%-50%) of FMS patients experience significant depression or anxiety, which may contribute to the severity of symptoms or result from having chronic pain. Most FMS patients experience both diurnal and seasonal variations in symptoms. Typically, symptoms are worse during periods of cold damp weather, at the beginning and end of the day, and during periods of emotional stress.”4
Several important distinctions emerged from the Copenhagen conference. First, the TeP of FMS was being differentiated from the trigger point (TrP) of myofascial pain syndrome. Second, results of muscle biopsies taken from TePs were inconclusive for any tissue abnormalities specific to FMS,5 and therefore the concept of FMS as a primary muscle disorder was falling out of favor. FMS was now being seen as a larger syndrome encompassing many symptoms that could be related back to increased sympathetic nervous system activity. Studies of the efficacy of various medications were showing that non-steroid, anti- inflammatory drugs (NSAIDs) and even corticosteroids did not have any significant effect on reducing the number of TePs in FMS patients,6,7 putting even more doubt on any “inflammatory” disorder of soft tissues. Yet, the interesting finding was that low doses of antidepressant medications did have a demonstrable, positive effect on TeP counts in some FMS patients, although this beneficial effect would prove to be short lived.8-10
As the complexity of fibromyalgia as a clinical syndrome eventually expanded from the 2 basic ACR criteria to include many other symptoms, no etiologic agent was ever identified as the underlying cause of this cluster of symptoms. This lack of any known etiologic agent is what led to the categorization of fibromyalgia as a syndrome rather than a disease. A syndrome is defined as “a running together; a concurrence of symptoms; an aggregate of signs and symptoms associated with any morbid process.”11 Like many other “syndromes” such as irritable bowel syndrome, restless legs syndrome, and irritable bladder syndrome, FMS has become a diagnosis of exclusion for patients in whom the etiology of the symptoms is unknown.
It is our opinion that the original premise of FMS as representing one grand, all-encompassing clinical syndrome is flawed. We propose that FMS is an oversimplified classification scheme that lumps together several distinct conditions that all happen to share a common cluster of symptoms. We recognize that certain patients clearly fulfill the classic criteria of FMS and have a very pronounced central nervous system (CNS) dysfunction of unknown origin that causes abnormal central processing of sensory stimuli. We propose that these patients indeed have what we term “Classic FMS” or “True FMS.”
Any serious discussion of FMS must also take into account, and provide plausible explanation for, the numerous (albeit anecdotal) success stories of FMS remissions and cures coming from alternative health care practitioners. It is our hypothesis that these patients represent a completely separate and distinct population or subset, for which we pro- pose the term “Pseudo FMS.” In expanding our hypothesis we present a novel classification scheme that differentiates “Classic FMS” from various subsets of “Pseudo FMS”.
PATIENTS WITH WIDESPREAD PAIN: A VAST POTENTIAL FOR MISDIAGNOSIS
According to strict adherence to the ACR criteria,3 a definite diagnosis of FMS should only be made when no other medical disease can explain the symptoms. Yet we have seen scores of patients diagnosed with FMS who never had even a simple blood test taken to rule out anemia or hypothyroidism, which are 2 common conditions that result in symptoms of fatigue and muscle aches, respectively. We have also seen patients labeled with FMS who, after further laboratory testing, were found to have rheumatoid arthritis, ankylosing spondylitis, Lyme disease, lymphoma, and other occult carcinomas in the early stages, as well as many other diseases.
This failure to adequately examine and perform laboratory tests may lead to a falsely high rate of FMS diagnosis and may further skew the epidemiologic studies of the prevalence of FMS. In our opinion, the misdiagnosis of FMS is becoming a serious problem within the US primary care medical community.
Some patients diagnosed with FMS have visited alternative health care practitioners and anecdotally report relief from many of the symptoms associated with their FMS. Based on our clinical experience with hundreds of patients diagnosed with FMS, we have heard some people claim that various types of manual treatment applied to their TePs (which were probably TrPs) relieved all of their muscle pain. Others say that “cleansing diets” and other forms of nutritional or herbal remedies helped to alleviate their headaches, irritable bowel, and bladder symptoms. Rather than rejecting these reports with the a priori assumption that they are scientifically unsound, we believe that some investigation into these claims is in order.
On the other hand, we have examined many patients who appear to have widespread pain and a global reduction of pain thresholds, associated with pronounced fatigue, low energy, and typically, a sleep disorder. A large number of these patients were seen by a primary care physician, who in turn referred them to a rheumatologist, who rendered a diagnosis of FMS. These patients often did not respond well to any type of manual treatment, including chiropractic, physical therapy, or massage, and typically appeared to have chronic pain despite multiple treatment interventions from multiple health care providers.
Our clinical experience, coupled with an intense interest in following the FMS literature for the past 10 years has led us to ponder answers to the following questions:
- Why do some FMS patients seem to experience substantial and long-term relief with manual treatment, whereas others derive little or no benefit from such therapy?
- Why do some FMS patients benefit from low-dose anti- depressants, and yet others feel worse or experience no effect?
- Why do dietary manipulation, vitamins, and herbal remedies relieve the gastrointestinal symptoms and fatigue of some cases of FMS, but not all?
- Why are some patients misdiagnosed with FMS, when in reality they have an organic disease that could readily be found with appropriate diagnostic testing?
- Why do some patients experience dramatic “cures” of their FMS symptoms when placed on thyroid or estrogen replacement therapy?
To answer these questions, a paradigm shift is required in which we alter the traditional view of FMS as one grand syndrome. We
 propose the following new classification system as outlined in the Figure. The differential diagnosis of patients who present with widespread pain/tenderness and fatigue may be broken down into 2 diagnostic categories: (1) Classic FMS and (2) Pseudo FMS. The diagnosis of Classic FMS fits the patient who has a significant sleep disorder, brain injury, depression, anxiety syndrome, and/or some other type of central nervous system dysfunction that leads to abnormal processing of sensory stimuli. These patients are thought to be experiencing some type of central allodynia, in which their nervous systems seem to process normally non-painful sensory stimuli as being painful.12 This subset of patients probably led the early rheumatologists down the research path to look beyond the peripheral joints and soft tissues for a cause of their widespread pain. They also represent the patients who are more likely to respond reasonably well to low-dose antidepressant or anxiolytic medications, biofeedback, and various types of psychotherapy or desensitization techniques. The medical management of these patients is therefore focused on altering brain and CNS neurochemistry.
propose the following new classification system as outlined in the Figure. The differential diagnosis of patients who present with widespread pain/tenderness and fatigue may be broken down into 2 diagnostic categories: (1) Classic FMS and (2) Pseudo FMS. The diagnosis of Classic FMS fits the patient who has a significant sleep disorder, brain injury, depression, anxiety syndrome, and/or some other type of central nervous system dysfunction that leads to abnormal processing of sensory stimuli. These patients are thought to be experiencing some type of central allodynia, in which their nervous systems seem to process normally non-painful sensory stimuli as being painful.12 This subset of patients probably led the early rheumatologists down the research path to look beyond the peripheral joints and soft tissues for a cause of their widespread pain. They also represent the patients who are more likely to respond reasonably well to low-dose antidepressant or anxiolytic medications, biofeedback, and various types of psychotherapy or desensitization techniques. The medical management of these patients is therefore focused on altering brain and CNS neurochemistry.
The category of Pseudo FMS is derived from the Latin “pseudo,” which translates as “false.” It is our opinion that this category represents patients who were misdiagnosed with FMS when, in fact, they had some other cause for their widespread pain and fatigue. The various causes of Pseudo FMS allow for further subdivision into 3 subcategories: (1) organic diseases, (2) functional disorders, and (3) musculoskeletal disorders. All 3 of these subcategories represent other medical problems that have signs and symptoms similar to Classic FMS, which were missed on initial examination and led to a misdiagnosis of FMS rather than their true disorder. In our opinion, the anecdotal success stories of FMS cures represent patients who had 1 or more of these types of Pseudo FMS and not Classic FMS. Please review the Figure for a visual representation of this reclassification of the differential diagnosis of patients with widespread pain and fatigue.
It is difficult to read the FMS literature and practice in a clinical setting without recognizing a very distinct pattern of symptoms that describes what we term “Classic FMS.” Patients with Classic FMS typically do not sleep well at night, often awaken feeling fatigued, complain of low energy, and have an intolerance to heavy exercise. They state that they feel “crummy” from the moment they wake up to the moment they lie down, and they have a lowered pain threshold to pressure over multiple areas of the body. Often these patients have an associated clinical depression or anxiety disorder, which may be the result of having to live with chronic pain or the result of a comorbid condition.4
These patients have frustrated themselves and the multitude of physicians to whom they have presented over the course of several months or years in a futile attempt to get a definite clinical diagnosis. All laboratory tests come back with normal findings on these patients; rheumatoid factor, sedimentation rate, and other serologic tests are negative. Yet clinically, the patients present as if they have some sort of systemic disorder, such as rheumatoid arthritis. Often the patients end up in a rheumatology clinic as a last resort attempt at diagnosis.
This “Classic FMS” presentation probably represents the type of patient that led the early rheumatology pioneers to research other clinical mechanisms responsible for wide- spread pain and the eventual publication of the 1990 ACR Criteria. As early as the late 1970s, there was scientific evidence surfacing about the correlation between the number of TePs, known as the TeP index, and the quality of a patient’s sleep. Harvey Moldofsky, a Canadian psychiatrist, is widely acknowledged as the first researcher to publish findings linking nonrestorative sleep to the clinical symptoms of widespread pain and fatigue in FMS patients. Moldofsky and Scarisbrick1,2 examined the brain wave activity of FMS patients in a sleep laboratory by use of electroencephalogram (EEG), and found that FMS patients as a group had disruption of their deeper stages of sleep. More recently, Moldofsky published a brief review of the literature regarding sleep disorders and soft-tissue tender- ness.13
As a result of this research on sleep disorders and FMS, it was presumed that patients with FMS might show clinical improvement with respect to soft-tissue tenderness if the quality of their sleep was improved.9,10 This led to the prescription of low doses of various antidepressant medications in an effort to induce deeper sleep, which clinically seemed to help many patients with FMS (at least in the short term). Various antidepressant medications still tend to be the prescription of choice for the medical management of FMS symptoms.
Because FMS was a diagnosis that evolved from the rheumatology field, it should not be surprising to see the early use of NSAIDs with FMS patients, based on the premise that the widespread soft-tissue tenderness was from some unknown type of inflammation. Numerous clinical trials, including rigorous randomized placebo-matched control studies, have all failed to show any positive clinical benefit for NSAIDs over placebo for the management of wide- spread pain associated with FMS.7 Even the corticosteroids such as prednisone show no better results than placebo when given to FMS patients.6 Based on these studies, it appears that gross soft-tissue inflammation does not play a major role in the pathogenesis of FMS.
If not peripheral soft-tissue inflammation, what is the mechanism by which multiple areas of the body and various soft tissues seem to be extremely tender in the patient with Classic FMS? The concept of FMS as a type of central allodynia proposed by Russell12 suggests that the etiology of FMS is a neurochemical imbalance in the CNS. Allodynia is defined as a clinical situation in which pain results from a stimulus that should not normally be painful. Many clinical studies have shown abnormalities within the cerebrospinal fluid and serum of patients with FMS versus healthy controls, the most dramatic of which were increased cerebrospinal fluid levels of substance P and decreased serum serotonin levels.14-16 Most antidepressant medications raise levels of serotonin by various mechanisms (selective serotonin re-uptake inhibitors, monoamine oxidase inhibitors), providing one plausible explanation of why low doses of these drugs help some patients with FMS.
Three important clinical features of FMS make us question any peripheral soft-tissue etiology of this syndrome. First, no biopsy study of TePs has yet shown any primary abnormality of muscle, tendon, or other soft tissue that is unique and specific to patients with FMS.17,18 Second, an intriguing finding came from studies that attempted to com- pare pain thresholds over TeP sites in FMS with normal “control points” on the same subjects. The results showed that patients with FMS had globally-reduced pain thresh- olds, that is, they perceived pain at lowered thresholds of pressure over both the control points and the TePs.”19,20 Lastly, the data comparing groups of healthy controls and patients with FMS clearly showed that the FMS group had an across-the-board decreased pain threshold and greater self-rated disability level.21
Another interesting hypothesis comes from Crofford,22 who reviews the role of the hypothalamic-pituitary-adrenal stress axis in the development of FMS. Crofford makes the point that many patients with FMS report the onset of their symptom complex after a significant period of emotional stress or a specific traumatic event. The literature does show that patients with FMS self-report a higher level of daily perceived stress and that their symptoms are significantly aggravated by stress. Most of the symptoms that are seen associated with FMS, such as sleep disorder, headache, and irritable bowel, can be traced back to increased activity of the hypothalamic-pituitary-adrenal axis and sympathetic nervous system. The significant association of clinical depression and anxiety disorders with FMS also argues for a CNS etiology of this syndrome.
Clearly there is a particular type of FMS patient who presents with increased sympathetic nervous system function, anxiety and/or depression, and a history of poor sleep with associated fatigue and widespread soft-tissue tenderness. Before FMS was a diagnostic option, these patients would probably have been labeled as having a somatoform pain disorder or somatization disorder. Some studies have shown that some FMS patients show significant clinical improvement after successful completion of a course of cognitive psychotherapy and other psychologic counseling techniques.23-26 Yet some would question whether the depression associated with FMS is nothing more than a secondary response to living with chronic pain. As a group, patients with chronic low back pain tend to have a coexisting depression syndrome.
Even more intriguing are recent reports by Donaldson et al27 of EEG spectrum changes that are characteristic of FMS patients; more specifically, dominance of slow wave activity in the frontal lobe. Donaldson et al have published some preliminary data showing clinical improvement of patients with FMS after a course of EEG biofeedback treatment associated with reversible changes in these brain wave pat- terns. They have found that patients with FMS generally complain of decreased ability to concentrate, short-term memory difficulties, and problems with performing multiple tasks at one time. Collectively, these concentration difficulties found in patients with FMS have been termed “fibro-fog,” and Donaldson et al assert that increased frontal lobe slow wave activity is the cause of this “fibro-fog.”
The high degree of association between depression and anxiety, and FMS symptoms has led some to speculate that the category of Classic FMS should merely be placed under the umbrella of somatization disorders. In layman’s terms, these patients would be told “FMS is all in your head.” Ironically, the data show that, indeed, the cause of symptoms may literally be “in the head” of patients with FMS (ie, alterations of brain biochemistry and EEG activity). It is interesting to note that alterations of frontal lobe EEG activity have also been demonstrated in patients with viral dis- ease and chronic fatigue syndrome.28,29 The underlying mechanisms by which the EEG activity is altered in FMS patients in still uncertain. Goldstein30 theorizes that FMS and CFS are due to postviral damage to the limbic portion of the brain and pituitary-hypothalamic pathways. Donaldson et al27 make an association between closed head trauma or other brain injuries and the onset of FMS symptoms.
In summary, Classic FMS represents the category of patients who have some type of CNS abnormality of unknown origin that causes them to have disturbed sleep, fatigue, and a feeling of “aching all over” (widespread pain). These patients do not respond well to standard manual treatments, such as chiropractic, physical therapy, or massage, because their condition is not primarily caused by any abnormality in the muscles or joints; it is a state of global lowered pain threshold caused by abnormal brain processing of sensory stimuli. This has led Russell12 to redefine FMS as “Central Allodynia” and Donaldson et al to call FMS a type of “CNS Myalgia.”27 This presence of CNS dysfunction, “fibro-fog,” memory problems, lowered pain threshold, sleep disorders, and other brain-processing difficulties is what appears to be the major differentiating factor between the categories of Classic FMS and Pseudo FMS.
ORGANIC DISEASES MISDIAGNOSED AS FMS
Type 1, Pseudo FMS
In patients with generalized pain and fatigue, it is imperative to assess the patient for underlying disorders such as anemia, Lyme disease, hypothyroidism, inflammatory arthritides, auto-immune disorders, multiple sclerosis, and occult malignancy as possible etiologies. Most of this assessment comes in the form of serologic testing that can easily be performed in the physician’s office or through a local clinical laboratory. As simple as these screening tests may be, it is not uncommon for clinicians to fail to have any laboratory tests performed on their patient and still render a diagnosis of FMS to the patient. According to ACR guide- lines and criteria, a diagnosis of FMS should not be rendered until all laboratory tests come back negative and fail to detect an “organic” reason for the symptoms.
This failure to order laboratory tests is certainly becoming more commonplace as primary care clinics overflow with excessive patient volume and experience capacity problems. Managed-care policies continue to whittle away at the amount of time spent by physicians with their patients, and it is understandable that a patient with “routine complaints” of fatigue and widespread pain could be summarily dismissed by the busy primary care physician as having FMS. It has been our clinical experience that this scenario is especially prevalent when a middle-aged woman presents with these complaints; she is more likely to be given a diagnosis of FMS and a prescription for antidepressant medications than a prescription for laboratory studies.
A simple, rational approach to laboratory assessment of these patients includes an initial complete blood count (CBC) and erthyrocyte sedimentation rate (ESR) to confirm the presence or absence of systemic inflammation or infection. Obvious reasons for excessive fatigue, such as anemia, can be ruled out on the CBC by screening for low RBC, altered hemoglobin, and abnormal RBC indices such as MCV, MCH, and MCHC. If anemia is present, it should be determined whether there is an occult gastrointestinal bleed or a malabsorption syndrome by means of a stool analysis. The microscopic evaluation of leukocytes may reveal abnormal cells that may be indicative of more serious pathologic condition, such as leukemia or multiple myeloma, although these are rarely found in general practice. The common anemias and their causes are listed in Table 1.

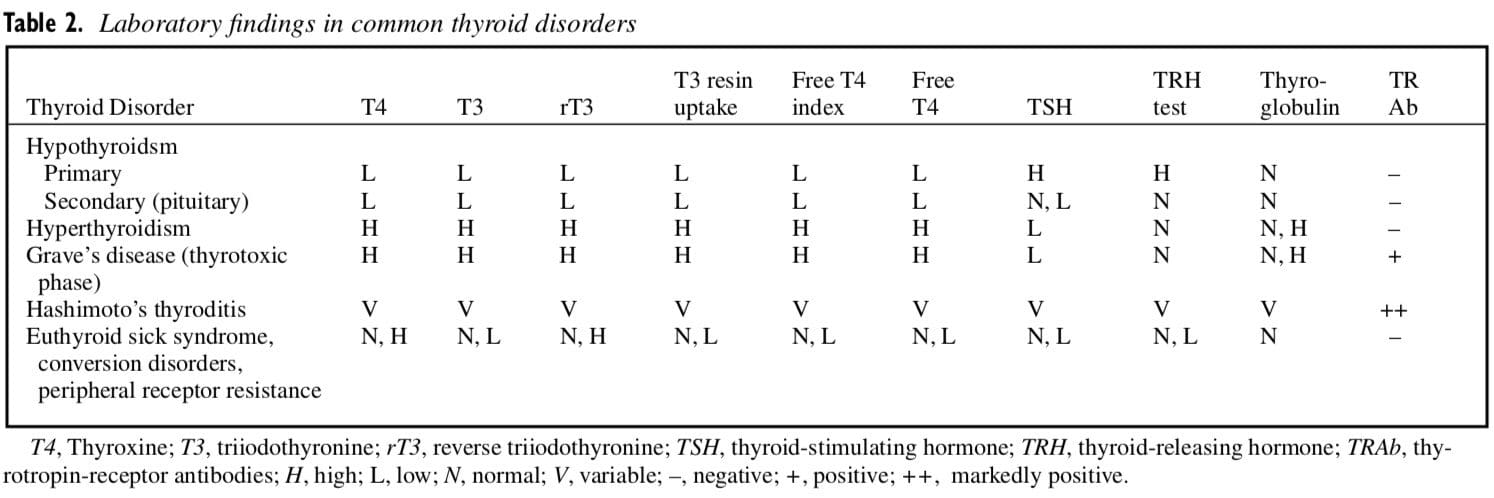
Thyroid function tests should also be done to rule out overt hypothyroidism as a cause of the patient’s symptoms.31,32 Various types of hypothyroid states exist, including the following: primary (disease of the thyroid gland itself), secondary or pituitary (from the lack of thyroid stimulating hormone), late Hashimoto’s thyroiditis (autoimmunity against the thyroid), iodine deficiency goiter, genetic thyroid enzyme defects, conversion of T4 to T3 defects, thyroid receptor insensitivity, and drug-induced hypothyroidism (ie, lithium, sulfonamides, phenylbutazone, or oral contraceptives).33-35 All of these disorders can result in a functional hypothyroidism and a very similar clinical presentation. Lowered function of the thyroid gland, regardless of the cause, can result in profound physiologic effects throughout virtually all systems of the body because of the effects of lowered temperature on enzyme function.
General signs and symptoms of low thyroid function include fatigue, weakness, cold intolerance, low morning axillary temperatures (normally 97.8°F to 98.2°F taken for 10 minutes before getting out of bed and averaged over a 5-day period), weight changes (usually weight gain), and depression.36 Common musculoskeletal signs and symptoms include muscle pain, stiffness, muscle cramping, muscle weakness, paresthesias, arthropathy, and sluggish deep tendon reflexes.37 Other reported musculoskeletal-related symptoms associated with hypothyroidism include adhesive capsulitis of the shoulders, proximal myopathy, carpal tunnel syndrome, and polyneuropathy that tends to be primarily sensory but some- times exhibits motor weakness as well.38,39 The incidence of musculoskeletal symptoms with hypothyroidism has been reported by Khaleeli, et al40 to be as high as 30% to 80%, depending on the special interests of the diagnosing physician. Many of these musculoskeletal symptoms are thought to result from myxedematous infiltration of ligaments and muscles. This is extremely important because it is precisely these vague musculoskeletal symptoms that may initially drive the patient with Pseudo FMS to the clinician. Many of these patients will likely be unaware that they have a thyroid condition, and if it is missed by the physician, their symptoms may inadvertently be misdiagnosed as Classic FMS.
The most useful serum laboratory tests to detect hypothyroidism are free T3, total T4, the free thyroxine index (FTI), and thyroid stimulating hormone (TSH).41,42 Laboratory findings in hypothyroidism may include a low or low normal T4 and free T3. TSH is usually increased in primary hypothyroidism because the pituitary attempts to increase thyroid output, but it is low or normal in secondary hypothyroidism (pituitary insufficiency). Total serum T3 is an unreliable test to detect hypothyroidism. Serum thyroperoxidase and thyroglobulin antibody titers are high only in cases of autoimmune processes causing hypothyroidism, such as in Hashimoto’s thyroiditis. Other associated laboratory findings of hypothyroidism may include hypercholesterolemia, increased liver enzymes, increased creatine kinase, hypoglycemia, albuminuria, and anemia.36,41,42
Serum studies often miss cases of mild hypothyroidism for several reasons, including the fact that patients with this condition tend to have low blood volume, which produces a concentration effect and results in thyroid hormones being interpreted as at normal levels when they are actually low. The TSH test, which would be expected to be high in cases of primary hypothyroidism, can also be falsely interpreted as showing normal results because a hypothyroid state may produce adverse cellular effects on the pituitary that result in decreased TSH production. T3 assays are of limited value because they cannot distinguish the difference between T3 and ineffectual reverse T3 (rT3) in patients with conversion disorders. Finally, it is uncertain how well-defined the nor- mal values used by clinical laboratories are for truly assess- ing thyroid function. Table 2 summarizes the various abnormal thyroid conditions that may be encountered in general practice. Lowe35 states that over 50% of patients with FMS have laboratory test results consistent with either primary or central hypothyroidism, and his textbook provides a comprehensive treatise on the subject of hypothyroidism and FMS.
It is often critically important to evaluate adrenal status in the patient with chronic fatigue because adrenal and thyroid function are so interdependent, and because increases in catacholamines and up-regulation of the sympathetic nervous system have been implicated in FMS, as previously discussed. Salivary tests that measure cortisol as well as dehydroepiandrosterone (DHEA) several times during the day can be beneficial in assessing hyperadrenal and adrenal exhausted states. Adrenal function is critical in the conversion of T4 to T3, which is 10 times more active than T4, in peripheral tissues. This conversion of T4 to T3 is influenced by adrenal cortisol, iron, selenium, B12, and magnesium. Too much cortisol in the system can increase conversion of T4 to an alternate form of T3 called reverse T3 (rT3). Reverse T3 is not recognized by peripheral thyroid hormone receptors and has little to no effect on cellular metabolism.43 Too little of the other nutrients listed above can result in a slowed conversion of T4 to T3. Therefore, borderline hypoadrenalism or hyperadrenalism can result in functional hypothyroidism, persistently low axillary temperatures, and fatigue even when the patient is taking significant dosages of lerothyroxine-based exogenous thyroid hormones. All female patients complaining of fatigue should test their axillary temperatures to rule out subtle forms of hypothyroidism that are often missed on standard thyroid blood tests, such as peripheral conversion disorders and peripheral resistance syndromes. This is particularly true if they are also com- plaining of muscle tenderness or other musculoskeletal symptoms.
Adrenal dysfunction may be addressed with stress reduction, proper sleep, and the use of nutrients such as vitamin C, vitamins B5, and B6, as well as adaptogenic herbs such as ginseng compounds, licorice root (glycyrrhiza glabra), withania (ashwagandha), and others.44,45 Stressful physiologic conditions such as pregnancy and trauma can induce a hypercortisol condition. Stressful situations in a patient’s life that are revealed during the medical history also commonly correlate with the onset of the patient’s thyroid- related symptoms and FMS. Often in these cases, the adrenal function is normalized when the stressor is removed, and the thyroid follows suit spontaneously.
Depressed liver function because of a toxic or overbur- dened liver can also influence the conversion of T4 to T3 via cytochrome P450 activity and result in low T3 levels. In general, the use of a combination of serum thyroid studies, salivary adrenal tests, and morning axillary temperatures is far superior to serum studies alone that may miss subtle cases of mild hypothyroidism.
The current medical treatment of choice for hypothyroidism is hormone replacement therapy with the drug levothyroxine (Synthroid [Knoll Pharm Co, Mt Olive, NJ]), which contains a synthetic version of T4. T4 is converted in the body to T3, the most active of the thyroid hormones.36 This certainly presents problems in patients with hypothyroidism caused by conversion defects. For some patients with very mild hypothyroid states, nutritional supplementation to support thyroid function and proper metabolism of thyroid hormones (L-tyrosine, iodine, selenium, B-vita- mins, and thyroid glandular concentrate) may provide enough therapy to avoid the need for hormone replacement therapy, or at least lessen the dosage required.44-46 Dosages of these nutrients must be adhered to strictly. Excessive thyroid glandular concentrate has been anecdotally reported to trigger autoimmune-type thyroid disorders in some cases, and iodine supplementation of more than 150 mg per day can suppress thyroid function. Monitoring with periodic laboratory assessment of thyroid function and axillary temperatures is required to assess the success, or lack thereof, of nutritional therapy.
Most cases of hypothyroidism will require the use of hor- mone-replacement medication. An alternative to the com- monly used pharmaceuticals such as Synthroid, Levothyroid (Forest Pharm, Inc, St Louis, Mo), and Levoxyl (Jones Pharm Co, St Louis, Mo) that only contain L-thyroxine (T4) is Armour thyroid (Forest Pharm, Inc, St. Louis, Mo). Armour thyroid is a pharmaceutical preparation of purified desiccated pork thyroid tissue that contains significant standardized levels of both T3 and T4, unlike the previously mentioned thyroid glandular nutritional supplements that contain no active hormone. It is commonly reported anecdo- tally to provide a smoother onset, less toxicity, and a better clinical and symptomatic response than synthetic com- pounds. This is particularly true in those patients who have T4 to T3 conversion disorders and often do not fare well on synthetic T4 (Synthroid) alone. The use of a combination of Levothyroxine and synthetic T3 therapy (Cytomel [Jones Pharm, Inc]) is also gaining popularity with many physicians for the management of patients who are refractive to T4 therapy alone and who have an aversion to using porcine thyroid preparations.
A standard blood chemistry panel is also recommended in order to evaluate overall systemic health, including serum fasting glucose, liver enzymes, and kidney function markers. However, without clinical evidence of diabetes, occult malignancy, arthritis, multiple sclerosis, or other systemic illness, serologic studies, such as rheumatoid factor, antinuclear anti- bodies, Borrelia burgdorferi, muscle enzymes, and serum complement, are generally not necessary.47 According to Hench, 32 Goldenberg, 47 and others, 10% to 15% of patients with FMS have isolated abnormal serologic test results with- out evidence of underlying connective tissue disease, which can often be misleading. This is where a detailed careful physical examination plays a large role. Only if the physical findings are suggestive of joint pain and inflammation are serologic studies such as standard rheumatoid panels and Lyme disease screening tests warranted.
Functional blood sugar abnormalities may not be detected merely with fasting blood glucose testing. If suspected, the clinician should consider adding glycosylated hemoglobin, as well as fasting and 2-hour postprandial glucose and insulin, to the laboratory analysis. This may detect dysglycemic conditions, including hyperinsulinemia and insulin resistance syndromes, as a possible cause for the patient’s fatigue. Because the brain requires about 25% of the circulating blood glucose to function properly, hypoglycemia will often cause symptoms of light-headedness, “foggy think- ing,” and sometimes frank syncope. These CNS symptoms mimic the “fibro-fog” described by patients with Classic FMS, explaining again how easily a misdiagnosis of Classic FMS could be made.
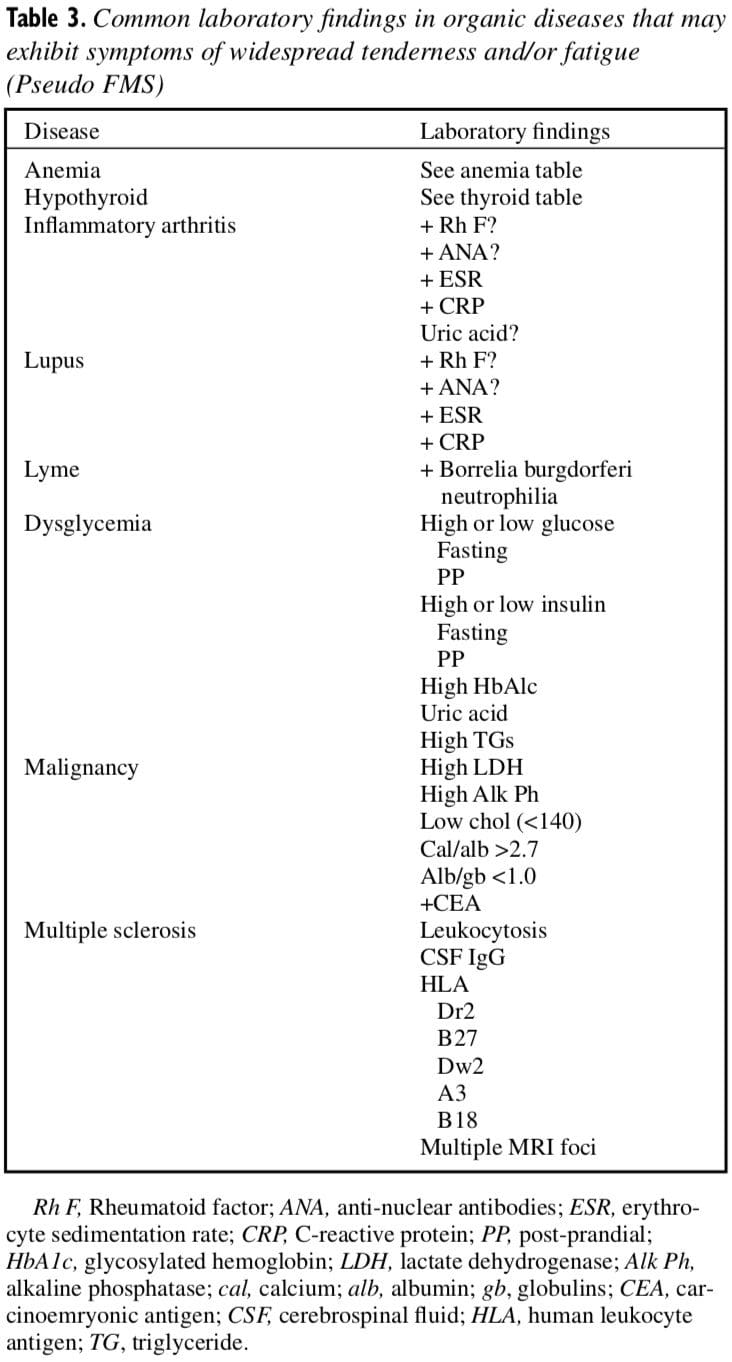
Again, it is important to note that if laboratory studies are positive for any of the above-noted “organic disorders,” a diagnosis of primary FMS is inappropriate. Stated bluntly, patients who have organic diseases that go undetected because of a shoddy examination are likely candidates for a misdiagnosis of Classic FMS. As a general rule, no patient should ever be given a diagnosis of FMS without a complete physical examination and screening laboratory testing to rule out the conditions listed in Table 3.
FUNCTIONAL DISORDERS MISDIAGNOSED AS FMS
Type 2, Pseudo FMS
The “functional” category of Pseudo FMS represents var- ious types of subclinical disease states and disorders involving dysfunction of internal organs, rather than true pathologic conditions. These functional disorders range from simple vitamin and mineral deficiencies to intestinal dysbiosis, gastric and pancreatic enzyme deficiencies, cellular dehydration, subtle endocrine imbalances, and post-viral immune suppression. All of these functional disorders have the common denominator of causing symptoms of low energy, fatigue, and/or widespread pain.
Several nutritional deficiencies have been identified in patients with fatigue and widespread tenderness, in whom supplementation with various nutrients (B-vitamins, magnesium, and malate) has shown positive results.48-50 Magnesium is the most common co-factor in enzymatic reactions in the body and, along with the B-vitamins, is of particular importance in the aerobic metabolic reactions of the Krebs cycle. Magnesium is also competitive with aluminum, a substance that is toxic at high levels and has been shown to be elevated in some patients diagnosed with FMS. Malic acid (malate) is a key Krebs cycle intermediate molecule, as well as being a potent aluminum detoxifier. Malate will result in increased urinary excretion of aluminum when given in therapeutic dosages to many patients with a diagnosis of FMS. In mild to moderate cases of fatigue and widespread pain, supplementation with these nutrients may have a significantly positive clinical effect. However, patients with severe fatigue usually do not respond adequately to these supplements alone, and require a more comprehensive functional approach.
The work of Bland and Bralley,51 Rigden,52,53 Cheney and Lapp,54 and others55-57 in the treatment of chronic fatigue syndrome has also been successfully used in limited case studies in the treatment of patients with FMS-like symptoms. This functional approach is centered on the premise that a breakdown of the intestinal mucosa caused by the chronic ingestion of processed foods, food- and water-based toxins, and the use of common over-the-counter drugs, such as NSAIDs, can lead to a hyperpermeable intestinal mucosa or “leaky gut syndrome.” This intestinal hyperpermeablility can result in the intestinal mucosa failing to act as a selective barrier, thereby allowing food toxins and partially digested food proteins to cross through the intestinal mucosa into the systemic blood supply. Over time, this increased antigenic and toxic load can lead to multiple acquired food allergies and put increased stress on the liver and its ability to adequately detoxify these substances through phase I and II pathways, ultimately resulting in increased tissue toxicity. Many of these patients are also on multiple prescriptions and over-the-counter medications, which also contribute to the liver burden.
This increased tissue toxicity and oxidative stress is thought to be a trigger for mitochondrial dysfunction—an inability of the body’s cells (particularly muscle cells) to efficiently use oxygen-dependent aerobic metabolic path- ways that account for the majority of adenosine triphosphate production. Decreased cellular adenosine triphosphate production can account for many of the symptoms and signs associated with FMS, including cognitive dysfunction, fatigue, and muscle pain caused by the build-up of anaerobic metabolites such as lactic acid. Treatment is therefore centered around repairing the intestinal mucosa, correcting any intestinal dysbiosis, and providing substances to the body that may aid tissue detoxification, allowing a return to normal cellular metabolism.
Therapy is preceded by physical examination and stan- dard laboratory assessment, as discussed previously. Assess- ment of intestinal health and the functional reserve of the liver and its detoxification abilities is then performed. This is commonly done with the help of functional laboratory stud- ies, such as the lactulose/mannitol challenge for evaluating intestinal permeability, and the complete digestive stool analysis (CDSA) for detecting markers of digestion, absorp- tion, and colonic flora.
The detoxification ability of the liver may partially be assessed by the salivary caffeine clearance and the acetaminophen and aspirin conjugation metabolite tests, which evaluate Phase I (cytochrome P450) and Phase II (conjugation) pathways, respectively. These tests are not performed by standard clinical laboratories but are available through specialized laboratories that offer functional testing. Once the data are collected and evaluated, a treatment program can be selected that may include specific nutrients, such as L-glutamine, purified hypoallergenic rice proteins, inulin, pantothenic acid, and antioxidants to aid in the repair of the intestinal mucosa and to correct any hyperpermeability (“leaky gut syndrome”).
Digestion and absorption difficulties suggested on the CDSA can be treated with the temporary use of pancreatic enzymes and hydrochloric acid in patients without gastritis or ulcer. Dysbiosis, an imbalance of colonic flora, can be addressed by the administration of lactobacillus acidophilus and probiotics, such as fructooligosaccharides. Any pathogenic bacteria, yeast, or parasites detected on the CDSA should be treated with the prescription or natural agents suggested by the sensitivity tests on the CDSA. These may include nonprescription substances such as berberine, garlic, citrus seed extract, artemisia, uva ursi, and others. This pro- gram of gastrointestinal restoration is described by Bland and Bralley,51 Rigden,52 Cheney and Lapp,54 and others as the “Four R” approach. The Four Rs of gastrointestinal restoration are the following: Replace (digestive enzymes and HCL), Repopulate (lactobacillus acidophilus, bifidobacteria, and fructooligosaccharides), Remove (eradicate any pathogenic microflora or parasites with the herbals suggest- ed by sensitivity tests on the CDSA, and remove allergenic foods from the diet), and Repair (L-glutamine, antioxidants, inulin, glutathione, N-acetylcystein, and fiber).
Up-regulation of liver detoxification pathways can be attempted by providing nutrients that are used in Phase I bio- transformation and Phase II conjugation pathways, such as N- acetyl cysteine, methionine, cysteine, sodium sulfate, glycine, glutamic acid, glutathione, and antioxidant nutrients. Patients with elevated Phase I cytochrome P450-enzyme activity should be treated with antioxidant therapy before detoxification begins to slow the production of, and mitigate the damage from, highly toxic biotransformed intermediate molecules that increase oxidative stress on the body. This should all be combined with a diet that emphasizes fresh foods and eliminates processed and allergenic foods. This will reduce the patient’s dietary toxic load (exotoxins), whereas the intestinal program will reduce gastrointestinal derived toxins (endotoxins).
Following a modified diet that eliminates the ingestion of gluten and dairy containing foods, and discontinuing as many drugs as possible may also help during the detoxification process. Although a more comprehensive and complete discussion of this functional approach to gastrointestinal and liver health is beyond the scope of this article, referring to the cited literature may help to further clarify these procedures for the practicing clinician, although larger-scale clinical trials are needed.51-57 In summary, there appears to be a certain subset of patients with Pseudo FMS who do not show any positive laboratory findings indicative of overt organic pathology or disease, yet have significant functional deficits in certain organ systems. The functional approach to the treatment of these patients with Pseudo FMS is not centered around any one agent or modality as the curative, or even palliative, solution. It is holistically centered on the principle that restoration of proper cellular metabolism, through balancing the endocrine system, and the reduction of cumulative toxic load and oxidative stress to the body may allow normalization of mitochondrial respiration, cellular energy production, and ultimately, a reduction in the signs and symptoms of low energy, fatigue, and widespread pain.
MUSCULOSKELETAL DISORDERS MISDIAGNOSED AS FMS
Type 3, Pseudo FMS
There is a long history of confusion in the literature regarding the terminology for myofascial pain syndrome and fibromyalgia syndrome. For years it was commonplace to see authors interchange the terms “fibrositis,” “myositis,” “myofascitis,” “fibromyalgia,” and “myofascial pain” when describing soft-tissue pain syndromes. Worse yet, there was frequent misuse of the terms “trigger point” and “tender point.” It seemed that if a patient had more than one area of complaint, or if the pain pattern did not fit any dermatomal or “anatomical” distribution, the diagnosis of fibromyalgia syndrome was readily given. One of us58 published an article outlining these issues in an attempt to help clarify differential diagnosis between myofascial pain syndrome and fibromyalgia syndrome.
When leading authors in the field routinely confuse the TePs points of fibromyalgia syndrome with the discrete TrPs found in myofascial pain syndromes, it comes as no surprise that patients are misdiagnosed with FMS when, in fact, they have some other musculoskeletal pain generator. In a study of 252 consecutive patients referred to his clinic for treatment of FMS, Donaldson et al27 found that on complete physical examination, 95 patients had their “widespread pain” reproduced on digital pressure over primary TrPs and were completely relieved of all their complaints by a course of physical therapy and manual myofascial techniques. In this study the misdiagnosis rate was 38%; stated another way, 38% of these “patients with FMS” had a musculoskeletal cause for their symptoms (Pseudo FMS) and did not have true FMS.
At the heart of this confusion lies ignorance about the different types of referred pain phenomena that occur in the human body, which may lead the unwary clinician toward an assumption that the presenting “nonanatomicical” pain pat- tern is “widespread pain” per the ACR criteria. It is routine to find distal referred pain phenomena arising from various deep somatic tissues, such as facet joints, spinal ligaments/muscles, intervertebral disks, meninges and dura mater, and joint capsules of the hip and shoulder. All of these tissues can be primary generators of noxious stimuli that cause the brain to perceive pain as arising from a location that is different from, or remote to, the somatic tissue from which this stimulus arises.
However, most of the referred pain phenomena caused by irritated somatic tissues have some type of regional pattern; that is, the shoulder joint refers pain in and around the shoulder, and distally into the upper extremity. According to strict interpretation of the ACR criteria, “widespread pain” is defined as pain that is bilateral, in the torso, and in both upper and lower extremities. We have seen numerous patients misdiagnosed with FMS based on faulty conclusions about what constitutes “widespread pain.” These patients need a clinician who will take a little time to sort out whether they truly “ache all over” and have widespread pain per the ACR criteria, or if, in fact, they have some other type of somatic referred pain pattern that merely appears to be widespread pain.
Many times patients have difficulty explaining or verbalizing what they are experiencing on a sensory level in their bodies. They have difficulty describing their pain unless they are specifically asked to use words such as “burning,” “throbbing,” “jabbing,” or the like. In addition, when the clinician is in a rush or behind schedule in this busy era of managed care, the patient often feels pressure to speak quickly. This scenario leads the patient to blurt out, “Well, I don’t know exactly where it hurts; I just hurt everywhere.” An incorrect assumption may be made by the clinician at this point, and a preliminary diagnosis of FMS given without delving deeper into the patient’s history or attempting to reproduce the pain pattern on physical examination.
This scenario is even further confounded by patients who have more than one pain generator, which will cause multiple (and hence confusing) overlapping regional pain patterns that get misinterpreted as global or widespread pain. Regional pain patterns are not characteristic of FMS; they are quite characteristic of pain generation by various irritated musculoskeletal tissues. The hallmark of all referred pain phenomena is a presentation of diffuse, nonspecific pain that is poorly localized. To the unwary clinician who is not well- versed in musculoskeletal diagnosis, these patterns may escape recognition in the differential diagnosis of FMS.
It should be rather simple to rule out the regional referred pain patterns caused by irritation or compression of peripheral nerves and spinal nerve roots. For example, in the case of median nerve involvement with carpal tunnel syndrome, the patient has a very distinct pattern of altered sensation in the hand and first 3 digits, with occasional referral of pain up to the elbow. In the case of nerve root impingement from spinal lesions, such as herniated disks, osteophytes, or later- al recess stenosis, the referred pain pattern follows a well known dermatomal distribution and is often recognized as such. In addition, nerve root irritation often has associated signs and symptoms such as gross motor weakness, true sensory loss, and diminished reflexes. These patients are rarely diagnosed with FMS because of the obvious nature of their regional pain pattern.
Less obvious are the regional pain patterns of patients who present with one (or a combination) of the following 3 types of referred pain phenomena: myofascial referred pain, scleratogenous referred pain, and dural referred pain. All of these referred pain patterns are characteristic of the somatic tissues from which they derive their names.
Myofascial referred pain59 arises from muscles that have been injured or have developed TrP activity. This type of pain is often described as “diffuse, deep, and achy” and can be reproduced by digital pressure applied directly over the offending myofascial TrP. When several muscles with multiple TrP are present, their nondermatomal referred pain complex could easily be mistaken for the widespread pain and tenderness found in FMS.
Scleratogenous referred pain60 arises from irritation of the somatic tissues surrounding deep joints—especially joint capsules, intervertebral disks, and articular ligaments. The spinal facet, hip, and shoulder joints are the pain generators most frequently seen clinically. These patients describe their pain as “very deep, dull, achy, and vague.” They will also state that with certain movements or motions they may experience a very “sharp, stabbing pain” that is rather localized, in addition to the previously noted diffuse pain. Exact reproduction of symptoms often occurs when the examiner stresses the joints by taking them to full end range position, by either passive mobilization or active range-of-motion testing.
Dural referred pain61 arises from irritation of the dura mater or meninges, and is frequently found in association with herni- ated disks that impinge on the thecal sac. This type of pain is often described as “nauseating or sickening” and can be intense enough to cause a patient to lose consciousness. This type of referred pain is also vague and ill-defined—felt in the mid-thoracic/posterior scapulae region with herniated cervical disks and in the lumbosacral/buttock region with herniated lumbar disks. The pain may also be referred in a vague pattern into the upper arm or thigh, but no further distally unless the spinal nerve roots are also affected.
An overarching principle of musculoskeletal diagnosis can be summed up by the following adage: reproduce the patient’s pain pattern and symptoms by physical examination. It should be axiomatic that if there is a pain generator arising from a somatic tissue, placing that tissue under mechanical stress or strain will elicit a painful response and reproduce the referred pain pattern. Furthermore, whenever a clinician can successfully reproduce a regional pain pat- tern on physical examination, the patient should not be diagnosed with FMS. By strict definition of the ACR criteria, these patients do not have widespread pain.
This category of musculoskeletal disorders that mimic FMS explains how some patients are “cured of their FMS” by physical therapy, chiropractic, exercises, massage therapy, or any other manual therapy. In fact, they had a regional pain syndrome that was misinterpreted as widespread pain and were subsequently misdiagnosed as having Classic FMS. The reason the patient responded clinically was because of the discovery of a specific pain generator, such as a myofascial TrP, joint dysfunction, or disk lesion, that responded well to some type of manual or mechanical therapy.
DISCUSSION
The present literature clearly suggests that Classic FMS is not a primary soft-tissue disorder and more likely represents a globally reduced pain threshold caused by central allodynia. The lowered threshold to pain is caused by abnormalities of CNS processing of sensory stimuli by the brain, and is not caused by any primary muscle or soft-tissue dysfunction. This abnormality of CNS function appears to be the key differentiating factor between the Classic and Pseudo FMS categories we have proposed in this article. Patients with Pseudo FMS do not have a primary CNS disorder; rather, they have some type of dysfunction of visceral or somatic organs as the underly- ing cause of their symptoms of widespread pain and fatigue.
Without becoming too metaphysical, it is difficult to avoid the question of where the line must be drawn that differentiates the brain/CNS processing disorders from the visceral/somatic disorders of the body. For example, thyroid hormone and blood sugar abnormalities can profoundly affect brain function. Conversely, increased limbic system and hypothalamic-pituitary-adrenal axis function can dramatically affect intestinal motility, heart rate, skeletal muscle tone, and other bodily systems through activation of the sympathetic and parasympathetic nervous systems. It seems that in some cases, primary treatment applied to various organ systems or musculoskeletal structures or both can have a dramatically positive clinical effect on certain patients with Pseudo FMS. On the other hand, treatment applied to the CNS through antidepressant medications, EEG biofeedback, and psychotherapy may diminish the widespread tenderness and TeP count in other patients with Classic FMS.
Several open questions about FMS still remain unanswered and are worthy of discussion. If Classic FMS truly represents a new disorder of brain biochemistry or CNS dysfunction, what is the etiologic agent that initiates the onset of the syndrome? Furthermore, what mechanism perpetuates the syndrome? How do we explain the high correlation of depression and anxiety found in FMS patients; are they causal or comorbid clinical phenomena?
There is also the curious statistical finding that FMS is 10 to 20 times more common in the female population. What is the explanation for this finding? Certainly, one is tempted to look at the menstrual cycle and hormonal changes as being possible etiologic agents; however, the data are lacking at this time regarding any specific hormonal abnormality unique to female patients with FMS. This area is ripe for future research studies.
We acknowledge that our proposed distinctions between Classic and Pseudo FMS, as well as the subsets of Pseudo FMS, are speculative and hypothetical. We do not claim to have found the “holy grail” regarding the appropriate diagnostic criteria for the classification of FMS as a diagnostic entity. Our sole motivation in writing this article is to attempt to provide clarification and finer distinctions about what we see in clinical practice as many subtypes of FMS. If our theory about multiple subtypes of Classic and Pseudo FMS is correct, it helps to explain why so many different specialities are involved with the diagnosis and treatment of these patients.
We recognize that our categories of “organic” and “functional” Pseudo FMS are arbitrary, and that some may find this distinction redundant. However, we see a clear distinction in clinical practice, whereby the “organic” disorders are often diagnosed and treated by physicians with standard medical procedures and medications, whereas the more subtle “functional” disorders are being diagnosed and treat- ed by alternative practitioners who use nutritional and herbal therapies. Essentially these 2 categories could be regarded on a single continuum of visceral dysfunction, with disorders of function at one end and frank pathologic conditions at the other end.
CONCLUSION: Fibromyalgia Syndrome
In conclusion, we make a plea to clinicians of all disciplines to study the FMS literature carefully and become well-versed in the nuances of this condition. It is our strong opinion that not all patients with widespread pain and fatigue fit the classic definition of FMS per the ACR criteria. We believe that all clinicians who treat these patients should be aware of the possibility that several subsets of patients with FMS probably do exist, with each type requiring very different types of diagnostic testing and treatment procedures. Furthermore, we believe in the old adage that “proper diagnosis is half the cure.” We hope that our pro- posed classification scheme of Classic and Pseudo FMS helps enable practitioners to more appropriately determine the cause of their patient’s symptoms, which will hopefully lead to more appropriate treatment choices and better clinical outcomes.
Michael J. Schneider, DC Private practice of Chiropractic 1720 Washington Road, Suite 201 Pittsburgh, PA 15241
David M. Brady, DC Chair, Department of Clinical Sciences University of Bridgeport College of Chiropractic Assistant Professor of Clinical Sciences University of Bridgeport College of Naturopathic Medicine Private practice of Chiropractic and Clinical Nutrition Orange, Connecticut
[/et_pb_text][et_pb_accordion _builder_version=”3.0.95″][et_pb_accordion_item _builder_version=”3.0.95″ title=”Blank” use_background_color_gradient=”off” background_color_gradient_start=”#2b87da” background_color_gradient_end=”#29c4a9″ background_color_gradient_type=”linear” background_color_gradient_direction=”180deg” background_color_gradient_direction_radial=”center” background_color_gradient_start_position=”0%” background_color_gradient_end_position=”100%” background_color_gradient_overlays_image=”off” parallax=”off” parallax_method=”on” background_size=”cover” background_position=”center” background_repeat=”no-repeat” background_blend=”normal” allow_player_pause=”off” custom_css_main_element=”display:none;” /][et_pb_accordion_item _builder_version=”3.0.95″ title=”References:” use_background_color_gradient=”off” background_color_gradient_start=”#2b87da” background_color_gradient_end=”#29c4a9″ background_color_gradient_type=”linear” background_color_gradient_direction=”180deg” background_color_gradient_direction_radial=”center” background_color_gradient_start_position=”0%” background_color_gradient_end_position=”100%” background_color_gradient_overlays_image=”off” parallax=”off” parallax_method=”on” background_size=”cover” background_position=”center” background_repeat=”no-repeat” background_blend=”normal” allow_player_pause=”off”]
1. Moldofsky H, Scarisbrick P. Induction of neurathenic musculoskeletal
pain syndrome by selective sleep stage deprivation.
Psycho Som Med 1976;38:35-44.
2. Moldofsky H, Scarisbrick P. Sleep and fibrositis syndrome.
Rheum Dis Clin North Am 1989;15:91-103.
3. Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C,
Goldenberg DL, et al. The American College of Rheumatology
1990 Criteria for the Classification of Fibromyalgia. Arthritis
Rheum 1990;33:160-72.
4. Consensus Document on Fibromyaglia: The Copenhagen Declaration.
J Musc Skel Pain 1993;1:295-312.
5. Schroder HD, Drewes AM, Andreasen A. Muscle biopsy in
fibromyalgia. J Musc Skel Pain 1993;1:165-9.
6. Clark SR, Tindall EA, Bennett RA. A double-blind crossover
trial of prednisone versus placebo in the treatment of fibrositis.
J Rheumatol 1985;12:980-3.
7. Goldenberg DL, Felson DT, Dinerman H. A randomized,
controlled trial of amitriptyline and naproxen in the treatment
of patients with fibromyalgia. Arthritis Rheum 1986;
29:1371-7.
8. Carette S, McCain GA, Bell DA, Fam AG. Evaluation of amitriptyline
in primary fibrositis. Arthritis Rheum 1986;29:
655-9.
9. Jaeschke R, Adachi J, Guyatt G, Keller J, Wong B. Clinical
usefulness of amitriptyline in fibromyalgia: the results of 23
N-of-1 randomized, controlled trials. J Rheumatol 1991;18:
447-51.
10. Bennett RM, Gatter RA, Campbell SM, Andrew SR, Clark
SR, Scarlo JA. A comparison of cyclobenzaprine and placebo
in the management of fibrositis. Arthritis Rheum 1988;31:
1535-42.
11. Stedman’s Medical Dictionary. Baltimore: Williams and Wilkins;
1976. p. 1378.
12. Russell IJ. Neurochemical pathogenesis of fibromyalgia syndrome.
J Musc Skel Pain 1996;4:61-92.
13. Moldofsky H. A chronobiologic theory of fibromyalgia. J
Musc Skel Pain 1993;1:49-59.
14. Russell IJ, Michalek JE, Vipraio GA, Fletcher EM, Javors MA,
Bowden CA. Platelet 3H-imipramine uptake receptor density
and serum serotonin levels in patients with fibromyalgia/
fibrositis syndrome. J Rheumatol 1992;19:104-9.
15. Russell IJ, Vaeroy H, Javers M, Nyberg F. Cerebrospinal fluid
biogenic amine metabolites in fibromyalgia/fibrositis syndrome
and rheumatoid arthritis. Arthritis Rheum 1992;35:550-6.
16. Russell IJ, Vipraio GA. Serotonin (5HT) in serum and platelets
from fibromyalgia patients and normal controls [abstract].
Arthritis Rheum 1994;37(Suppl):S214.
17. Yunus MB, Kalyan-Raman UP, Masi AT, Aldag JT. Electron
microscopic studies of muscle biopsy in primary fibromyalgia
syndrome: a controlled and blinded study. J Rheumatol
1989;16:97-101.
18. Bengtsson A, Henriksson KG, Larsson J. Muscle biopsy in primary
fibromyalgia: light microscopic and histochemical findings.
Scand J Rheum 1986;15:1-6.
19. Vecchiet L, Giamberardino MA, de Bigontina P, Dragani L.
Comparative sensory evaluation of parietal tissues in painful
and nonpainful areas in fibromyalgia and myofascial pain
syndrome. In: Gebhart GF, Hammond DL, Jensen TS,
editors. Proceedings of the 7th World Congress on Pain:
progress in pain and management. Seattle: IASP Press; 1994.
p. 177-85.
20. Graven-Nielsen T, Sörenson J, Henriksson KG, Bengtsson M,
Arendt-Nielsen L. Central hyperexcitability in fibromyalgia. J
Musc Skel Pain 1999;7:261-71.
21. Roth RS, Bachman JE. Pain experience, psychological functioning
and self-reported disability in chronic myofascial pain
and fibromyalgia. J Musc Skel Pain 1993;1:209-16.
22. Crofford LJ. The hypothalamic-pituitary-adrenal stress axis
in the fibromyalgia syndrome. J Musc Skel Pain 1996;4:
181-200.
23. Kogstad O, Hintringer F. Patients with fibromyalgia in pain
school. J Musc Skel Pain 1993;1:261-5.
24. White KP, Nielson WR. Cognitive behavioral treatment of
fibromyalgia syndrome: a follow-up assessment. J Rheumatol
1995;22:717-21.
25. Kaplan KH, Goldenberg DL, Galvin-Nadeau M. The impact of
a meditation-based stress reduction program on fibromyalgia.
Gen Hosp Psych 1993;15:284-9.
26. Bradley LA. Cognitive behavioral therapy for fibromyalgia. J
Rheumatol 1989;16(Suppl):131-6.
27. Donaldson CS, Sella GE, Mueller HH. Fibromyalgia: a retrospective
study of 252 consecutive referrals. Can J Clin Med
1998;5:116-27.
28. Billiot K, Budzynski T, Andrasik F. EEG patterns and chronic
fatigue syndrome. J Neurotherapy 1997;2:20-30.
29. Goldenberg DL. Fibromyalgia and its relation to chronic
fatigue syndrome, viral illness, and immune abnormalities. J
Rheumatol 1989;16(Suppl):91-3.
30. Goldstein JA. Chronic fatigue syndromes: the limbic hypothesis.
Binghamton (NY): Haworth Medical Press; 1993.
31. Bennett RM. Confounding features of fibromyalgia syndrome:
a current perspective of differential diagnosis. J Rheumatol
1989;16:58-61.
32.Hench PK. Evaluation and differential diagnosis of fibromyalgia:
approach to diagnosis and management. Rheum Dis Clin
North Am 1989;15:19-29.
33. Berkow R, Fletcher AJ, editors. The Merck manual. 16th ed.
Rahway (NJ): Merck & Co; 1992.
34. Guyton AC, Hall JE. Textbook of medical physiology. 9th ed.
Philadelphia: W.B. Saunders; 1996.
35. Lowe JC. The metabolic treatment of fibromyalgia. Boulder
(CO): McDowell Pub; 2000.
36. Tierney LM, McPhee SJ, Papadakis MA, editors. Current medical
diagnosis and treatment. 38th ed. Stamford (CT): Appleton
& Lange; 1999.
37. Golding DN. Hypothyroidism presenting with musculoskeletal
symptoms. Ann Rheum Dis 1970;29:25-43.
38. Neeck G, Riedel W, Schmidt KL. Neuropathy, myopathy, and
destructive arthropathy in primary hypothyroidism. J Rheumatol
1990;17:1697-700.
39. Bowman C, Jeffcoat WJ, Pattrick M, Doherty M. Bilateral
adhesive capsulitis, oligoarthritis, and proximal myopathy as
presentation of hypothyroidism. Br J Rheumatol 1988;27:
62-4.
40. Khaleeli A, Griffith DG, Edwards RH. The clinical presentation
of hypothyroid myopathy and its relationship to abnormalities
in structure and function of skeletal muscle. Clin Endocrinol
1983;19:365-76.
41. Fischbach F. A manual of laboratory and diagnostic tests. 6th
ed. Philadelphia: JB Lippincott Co; 2000.
42. Tilkian S, Conover M, Tilkian AG. Clinical implications of
laboratory tests. 3rd Edition. St. Louis (MO): Mosby; 1995.
43. Utiger RD. The thyroid: physiology, thyrotoxicosis, hypothyroidism,
and the painful thyroid. In: Felig P, Frohman LA, editors.
Endocrinology and metabolism. 3rd ed. New York:
McGraw-Hill; 1995. p. 435-19.
44. Balch JF, Balch PA. Prescription for natural healing. Garden
City Park (NY): Avery; 1990.
45. Werbach MR. Nutritional influences on illness. 2nd ed.
Tarzana (CA): Third Line Press; 1996.
46. Grabowski RJ. Current nutritional therapy: a clinical reference.
San Antonio (TX): Image Press; 1993.
47. Goldenberg DL. Fibromyalgia syndrome: an emerging but
controversial condition. JAMA 1987;257:2782-7.
48. Abraham GE, Flechas JD. Management of fibromyalgia: rationale for the use of magnesium and malic acid. J Nutr Med
1992;3:49-59. 49. Cox IM, Campbell MJ, Dowson D. Red blood cell magnesium
and chronic fatigue syndrome. Lancet 1991;337:
747-60.
50. Domingo JL, Gomez M, Llobet JM. Citric, malic, and succinic
acids as possible alternatives to deferoxamine in aluminum
toxicity. Clin Toxicol 1988;26:67-79.
51. Bland J, Bralley A. Nutritional up-regulation of hepatic detoxification
enzymes. J Appl Nutr 1992;44:2-15.
52. Rigden S. Ultra Clear – chronic fatigue deficiency syndrome
study preliminary report. Technical bulletin. Seattle: Healthcomm,
Inc; 1994.
53. Rigden S. Entero-hepatic resuscitation program for CFIDS.
CFIDS Chron Spring 1995. p. 46-9.
54. Cheney PR, Lapp CW. Entero-hepatic resuscitation in patients
with chronic fatigue syndrome: a pyramid of nutritional therapy.
CFIDS Chron Fall 1993. p. 1-3.
55. Lanfranchi RG, Donovan PM, Deuster P, Jaffee R. Fibromyalgia,
chronic pain, and the “leaky gut” syndrome. Today’s
Chiropr 1994; Mar/Apr:32-39.
56. Rowe AH. Allergic fatigue and toxemia. Ann Allergy 1959;
17:9-18.
57. Pressman AH. Metabolic toxicity and neuromuscular pain,
joint disorders, and fibromyalgia. J Am Chiro Assoc 1993;30:
77-8.
58. Schneider MJ. Tender points/fibromyalgia vs. tender points/
myofascial pain syndrome: a need for clarity in terminology
and differential diagnosis. J Manipulative Physiol Ther 1995;
18:398-406.
59. Simons DG, Travell JG, Simons LS. Myofascial pain and dysfunction:
the trigger point manual. Volume 1, 2nd ed. Baltimore:
Williams and Wilkins; 1999.
60. Goodman CC, Snyder TE. Differential diagnosis in physical
therapy. Philadelphia: WB Saunders; 1990.
61. Cyriax J. Textbook of orthopedic medicine. Volume 1, 6th ed.
London: Balliere and Tindall; 1975.
[/et_pb_accordion_item][et_pb_accordion_item _builder_version=”3.0.95″ title=”Close Accordion” use_background_color_gradient=”off” background_color_gradient_start=”#2b87da” background_color_gradient_end=”#29c4a9″ background_color_gradient_type=”linear” background_color_gradient_direction=”180deg” background_color_gradient_direction_radial=”center” background_color_gradient_start_position=”0%” background_color_gradient_end_position=”100%” background_color_gradient_overlays_image=”off” parallax=”off” parallax_method=”on” background_size=”cover” background_position=”center” background_repeat=”no-repeat” background_blend=”normal” allow_player_pause=”off” open_toggle_background_color=”#ffffff” closed_toggle_background_color=”#ffffff” custom_padding=”0px|||” custom_padding_tablet=”0px|||” custom_padding_phone=”0px|||” custom_css_main_element=”border:none;” custom_css_toggle_title=”font-size:0.8em;” custom_css_toggle_icon=”display:none;” /][/et_pb_accordion][/et_pb_column][/et_pb_row][/et_pb_section]
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card