


Title: The Efficacy of Chiropractic Adjustments in the care of Migraine Headache with patients presenting with cervical disc bulge.
Abstract: Objective: To explore the efficacy of chiropractic adjustments, and non-surgical spinal decompression in the treatment of cervical spine disc conditions presenting as neck pain, migraine headache, dizziness and visual disturbances. Diagnostic studies included physical examination, computer aided range of motion, orthopedic and neurological examinations, plain film x-ray studies, brain MRI, cervical spine MRI examinations. Treatments included specific spinal adjustments, low level laser therapy and spinal decompression. The patient’s outcome proved excellent in reduction of neck pain, headache severity and frequency as well as elimination of dizziness and visual disturbances.
Introduction: On 11/19/13 a 37-year-old female presented for examination and treatment of neck pain, migraine headaches with associated dizziness and visual disturbances. The patient denies and recent injuries.
Table of Contents
Presenting Concerns Of Research Study
The patient reports neck pain in the cervical occipital region as a 4 on the Verbal Analog Scale of 0 meaning the complete absence of pain and 10 being unbearable pain. The duration of the current symptom picture is 2 years and 1 month. The patient further reports episodic migraine headaches starting at the upper cervical region and progressing into her occipital area. These episodes are accompanied by dizziness and visual disturbances described as kaleidoscope vision. At the time of the initial consultation these episodes were occurring 2-3 times per week. The patient reports being afraid to drive her car due to concerns about headache onset. The patient reports past consultations with her medical doctor who diagnosed her with vertigo and previous chiropractic care without results. The records from both consultations were reviewed personally.
Clinical Findings: The patient presents with complaints of neck pain, headaches, dizziness and visual disturbances of 2 years duration. The patient is a 37-year-old female who is a mother of 2. The ages are 16 and 3.
Her vital signs are:
Height – 5 ft. 0 inches
Weight – 130 lbs.
Handedness – R
Blood Pressure – L – 107 systolic and 78 diastolic
Radial Pulse – 75 BPM
The patient’s Review of Systems and Family History were unremarkable.
Palpation/Spasm/Tissue changes: The patient was evaluated by palpation and observation with the following findings: Bilateral cervical spine spasms rated at +2 in the cervical-occipital region. Orthopedic testing was unremarkable. Range of motion examination revealed mildly decreased left lateral flexion, moderately decreased flexion, right lateral flexion and extension. No pain was produced during range of motion examination.
Neurological Examination: Biceps, Triceps and Brachioradialis reflexes were rated at a +2 bilaterally. Sensory examination revealed normal sensation bilaterally for dermatomes C-5 through T1. Motor/Muscle testing revealed 5 out of 5 bilaterally for Deltoids, Biceps, and Triceps, Forearm and Intrinsic Hand muscles.
Radiographic findings: reversal of the cervical curve with altered C5/C6 disc space is noted. (Fig. 1, (A) (B) A small osteophyte is observed on the posterior inferior body of C5. Flexion malposition of C5 is also noted. (Fig. 1, (B).
Fig. 1, (A), (B) show loss of the cervical lordosis, flexion malposition of C5, partial collapse of C5/6 anterior disc space.
 Fig. 1. (B) shows upon magnification a small posterior-inferior osteophyte.
Fig. 1. (B) shows upon magnification a small posterior-inferior osteophyte.
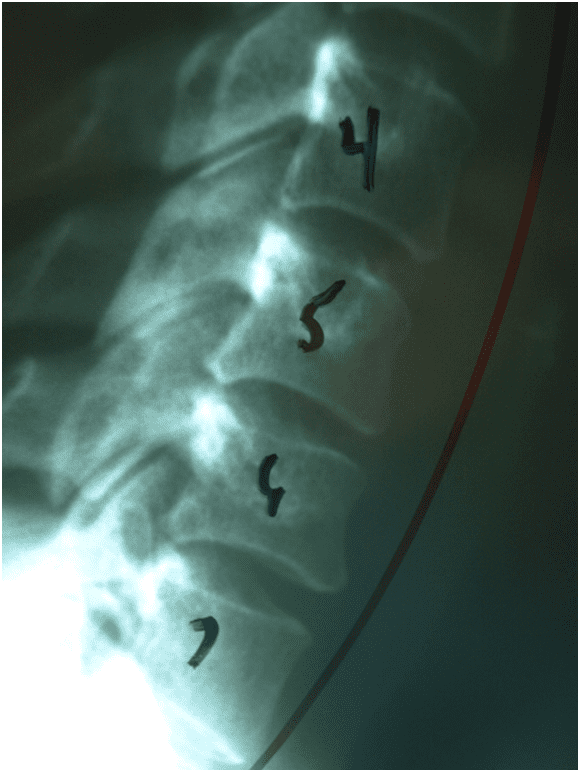
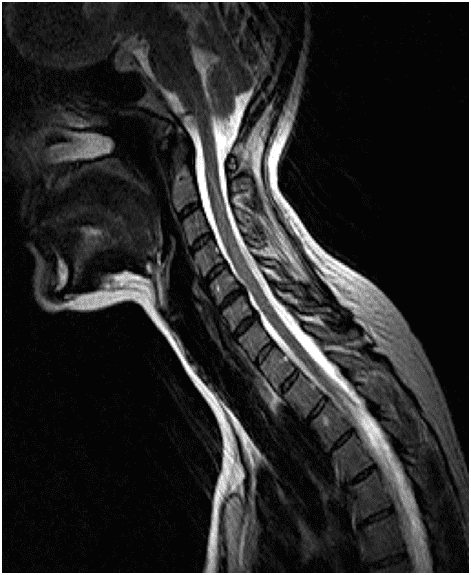
Fig. 2, (A), (B) shows in T2 MRI images (A) is Sagittal and (B) is Axial a C5/6 central disc herniation contacting the ventral cord.
Diagnostic Focus and Assessment: Diagnoses considered are: Brain Tumor, Cervical Disc Displacement, and Cervical-cranial syndrome. A brain MRI was ordered and produced normal findings. Diagnostic reasoning included the C5/C6 disc/osteophyte complex and the encroachment into the ventral aspect of the central canal and contact with the cervical spinal cord. (1) Peter J. Tuchin, GradDipChiro, DipOHS, Henry Pollard, GradDipChiro, GradDipAppSc, Rod Bonillo, DC, DO. Received 29 June 1999. Another consideration was the treatment schedule because the patient lives 60 miles west of the clinic and 2 treatments was the ordered therapeutic schedule.
Therapeutic Focus and Assessment: Assessment of the cervical spine MRI both sagittal and axial views of the C5/C6 and C6/C7 segmental levels revealed adequate space between the cervical cord and posterior vertebral elements. It was determined that conservative management of this patient was appropriate. Therapeutic focus was reducing the pressure of the C5/C6 disc/osteophyte complex on the ventral cord. Promoting healing of damaged nerve tissue and restoring more favorable position and motion of vertebral segments C5/C6. The modalities used to treat this patient were:
1. Specific Spinal Adjustments: utilizing a Sigma Precision Adjusting Instrument to introduce a percussive force of 20 lbs. with a maximum of impact number of 50.
2. Spinal Decompression: A Hill Spinal Decompression table was utilized with 8 lbs. of pull maximum and a cycle of 5 minute at maximum and 5 minutes at reduction to 50% over a 25 minutes treatment session. The patient completed 18 sessions in total.
3. Low Level Laser Therapy was used to promote healing on a cellular level using a Dynatron Solaris system. Treatments consisted of 30 seconds of exposure to an 860-nanometer beam at C5/C6 and C6/C7 levels.
Adjustments Follow-Up And Outcomes
The patient’s compliance to the treatment schedule as rated at 9 of 10. Completion of the recommended 18 treatments required 1 week longer than anticipated. For personal reasons the patient missed 2 treatment sessions but made them up by adding a week to the estimated completion date. Upon discharge examination the patient reports her neck pain on the Verbal Analog Scale a 2 of 10 with 0 being the complete absence of pain and 10 being the worst pain imaginable. She further reported her headaches as a 1 on the Verbal Analog Scale. Both symptoms were constant since 10/01/11. This is duration of 25 months prior to her first visit. Her symptoms of dizziness and visual disturbances have been absent since 12/13/13.
Discussion: Headaches and Migraine Headaches are a big health problem. It has been estimated that 47% of the adult population have headache at least once within last year in general. More than 90% of sufferers are unable to work or function normally during their migraine. American employers lose more than $13 billion each year as a result of 113 million lost workdays due to migraine. (2) Schwartz BS1, Stewart WF, Lipton RB. J Occup Environ Med. 1997 Apr; 39(4): 320-7.
This case report is very limited because it represents the experience and clinical findings for just 1 patient. However a study of the references included with this report as well as reports by care providers as well as testimonials from patients indicates that more study should be invested in the relationship of the cervical spine, its structures and biomechanics during the diagnostic workup on headache and migraine patients.
Informed Consent: The patient provided a signed informed consent.
Competing Interests: There are no competing interests writing of this case report.
De-Identification: All the patient’s related data has been removed from this case report.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 . 
References:
1. Schwartz BS1, Stewart WF, Lipton RB.
J Occup Environ Med. 1997 Apr; 39(4): 320-7.
Lost workdays and decreased work effectiveness associated with headache in the workplace.
Wikipedia, The Free Encyclopedia. (2010, July). Human musculoskeletal system. Retrieved from http://en.wikipedia.org/wiki/Musculoskeletal
2. Vernon, H., Humphreys, K., & Hagino, C. (2007). Chronic mechanical neck pain in adults treated by manual therapy: A systematic review of change scores in randomized clinical trials, Journal of Manipulative and Physiological Therapeutics, 30(3), 215-227.
3. Peter J. Tuchin, GradDipChiro, DipOHS, Henry Pollard, GradDipChiro, GradDipAppSc, Rod Bonillo, DC, DO. Received 29 June 1999
A randomized controlled trial of chiropractic spinal manipulative therapy for migraine☆
4.Mark Studin DC, FASBE (C), DAAPM, DAAMLP, William J. Owens DC, DAAMLP Chronic Neck Pain and Chiropractic. A Comparative Study with Massage Therapy.
5. D’Antoni AV, Croft AC. Prevalence of Herniated Intervertebral Discs of the Cervical Spine in Asymptomatic Subjects Using MRI Scans: A Qualitative Systemic Review. Journal of Whiplash & Related Disorders 2006; 5(1):5-13.
6. Murphy, D. R., Hurwitz, E. L., & McGovern, E. E. (2009). A nonsurgical approach to the management of patients with lumbar radiculopathy secondary to herniated disk: A prospective observational cohort study with follow-up. Journal of Manipulative and Physiological Therapeutics, 32(9), 723-733.
Additional Topics: Chiropractic Helps Patients Avoid Back Surgery
Back pain is a common symptom which affects or will affect a majority of the population at least once throughout their lifetime. While most back pain cases may resolve on their own, some instances of the pain and discomfort can be attributed to more serious spinal conditions. Fortunately, a variety of treatment options are available for patients before considering spinal surgical interventions. Chiropractic care is a safe and effective, alternative treatment option which helps carefully restore the original health of the spine, reducing or eliminating spinal misalignment which may be causing back pain.
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card