


Table of Contents
Acute Elbow Trauma
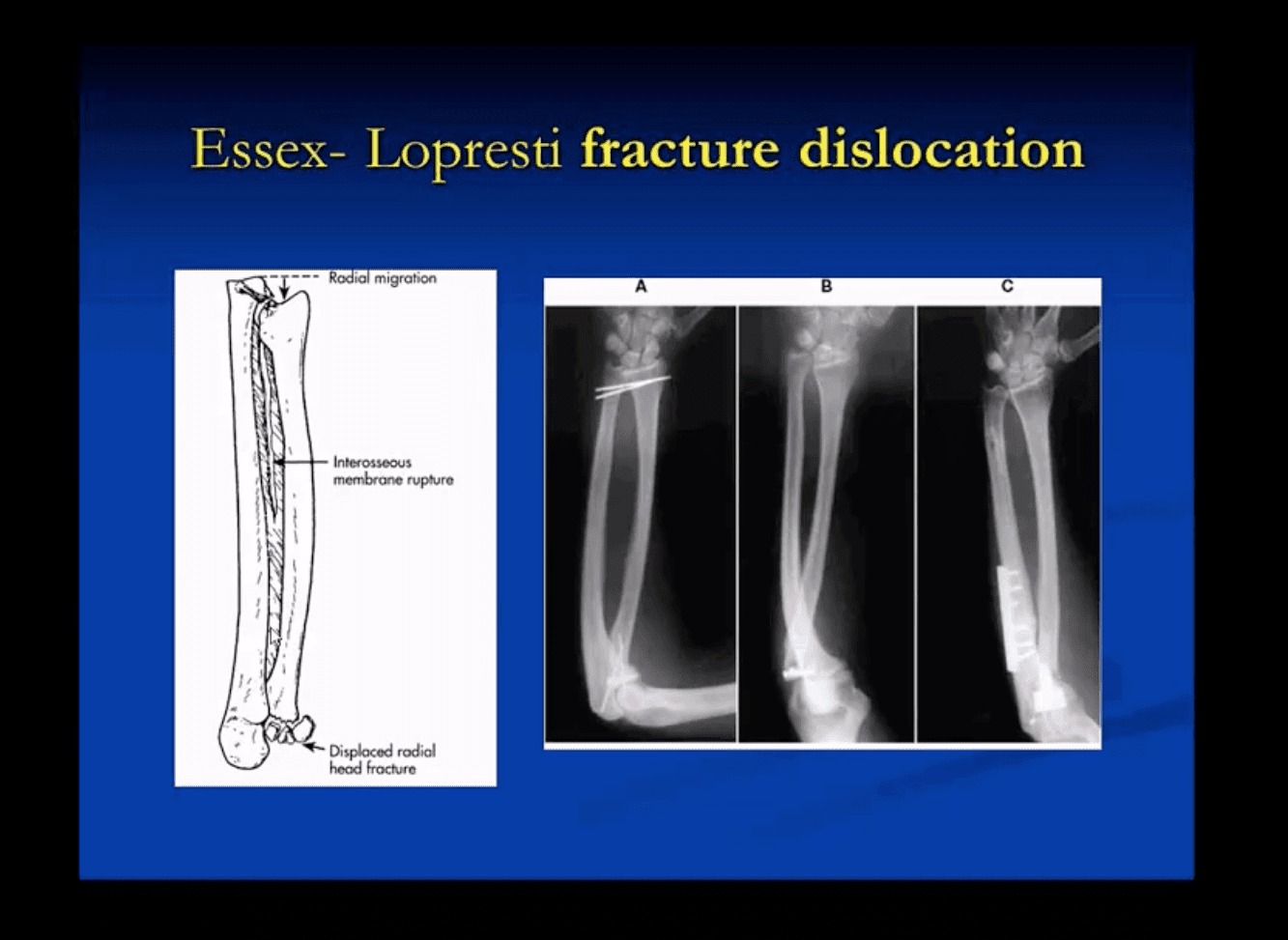
- In adults: Radial head Fx is the m/c (33%) and accounts for 1.5-4% of all fractures. Etiology: FOOSH with forearm pronated. Associated injuries: elbow collateral ligaments tears. EssexLoprestiFx with interosseous membrane tearing and dislocation of the Distal Radio-Ulnar Joint(DRUJ)
- Terrible triad: of the Radial head Fx, elbow dislocation and Coronoid process Fx (typically avulsed by the Brachialis M)
- Imaging: 1st step is x-radiography with elbow series, CT scanning may help in complex cases, MRIif ligamentous injury.
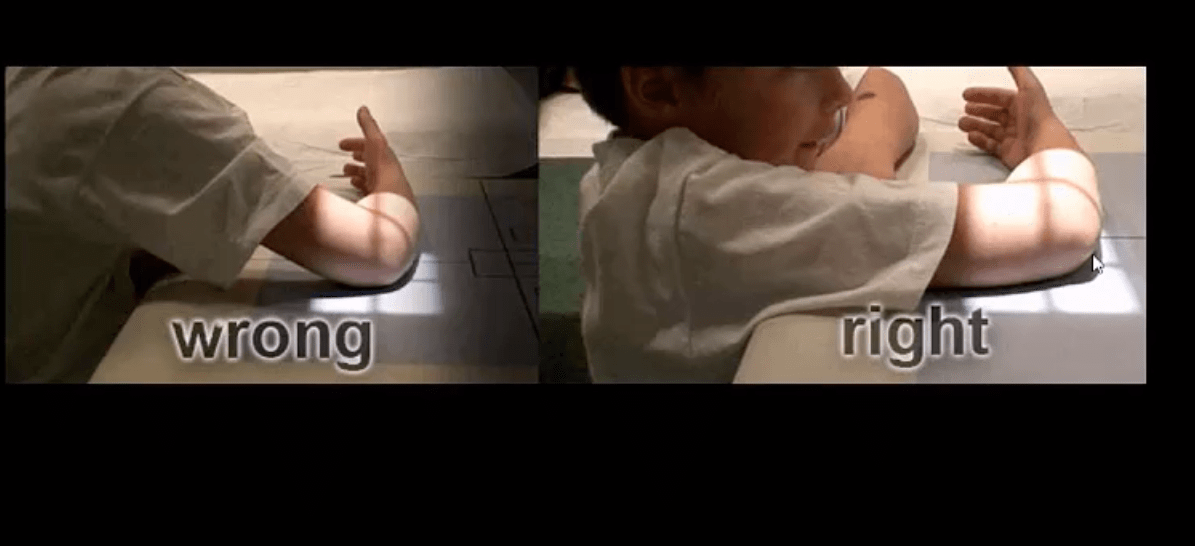
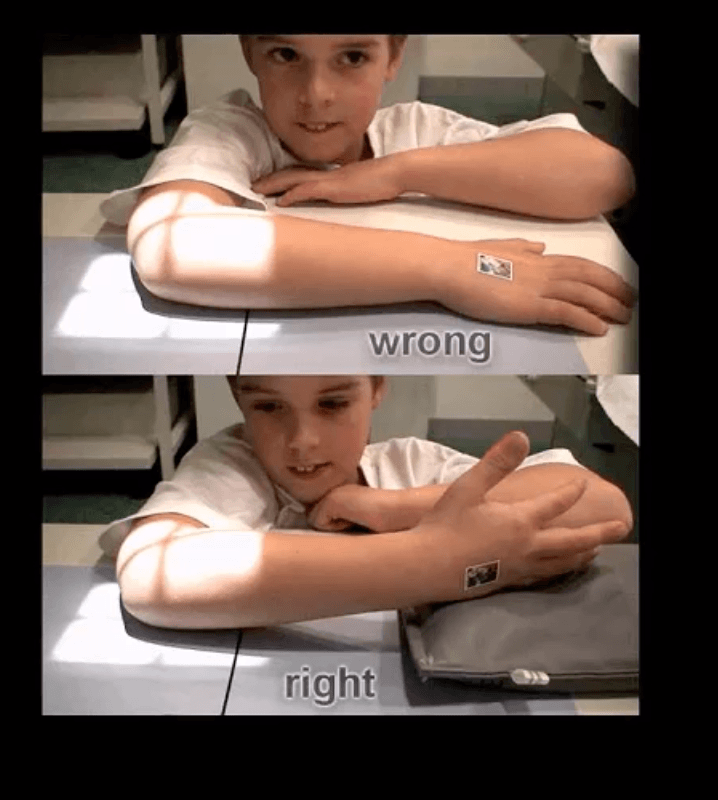
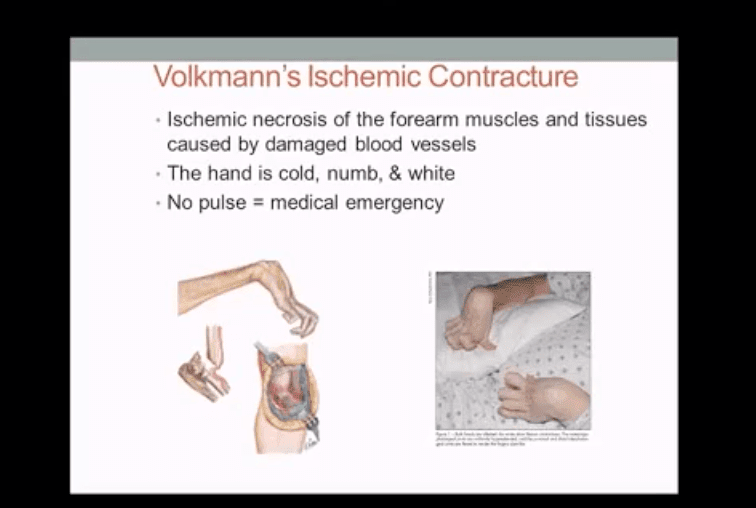
- In children: Supracondylar Fx of the distal humerus accounts for 90% of acute trauma. It is always d/t accidental elbow extended, rarely <5% with flexed elbow. MostSupracondylar Fx occur in children <10 y.o. Males>Females. Complications: malunion in cubitus varus aka Gunstock deformity, vascular injury and acute ischemic compartment syndrome with Volkmann contracture
- Imaging: 1st step x-radiography can be sufficient. CT occasionally used in complex cases.
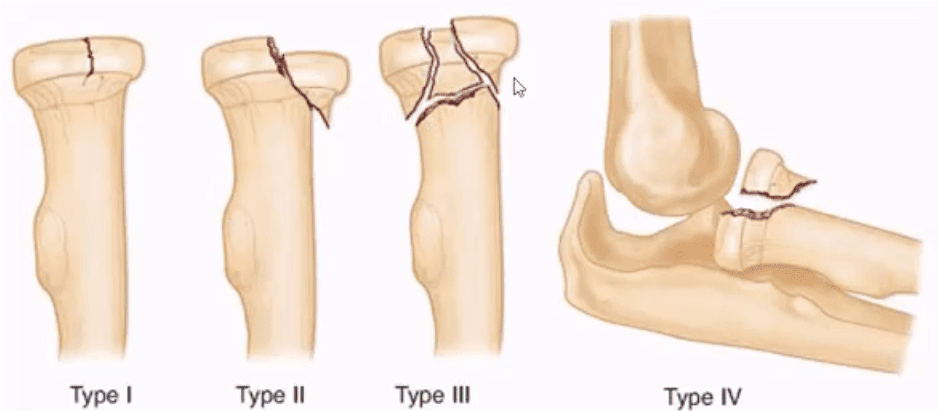
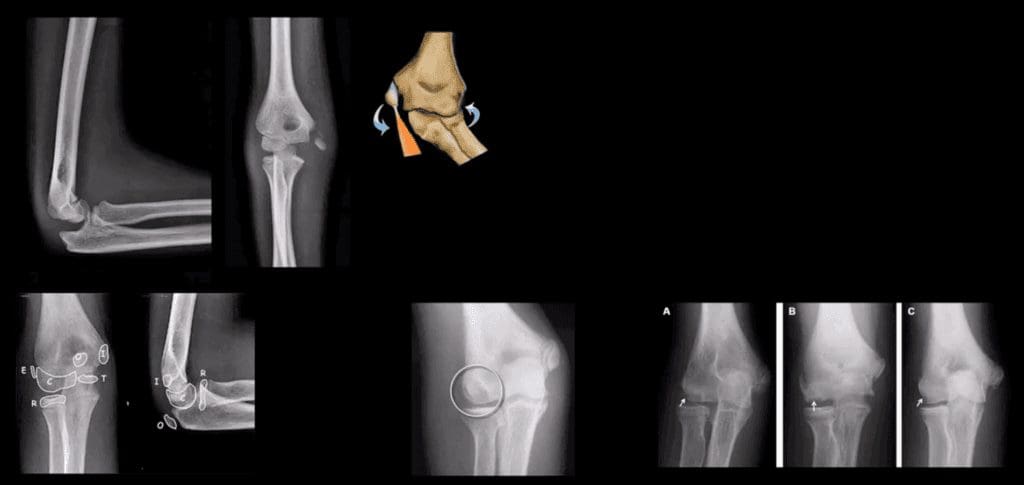
- Radial head (RH) Fx: Mason classification helps to determine the degree of complexity and mode of treatment
- Type 1- undisplaced is the m/c and stable contained by ligaments. On radiographs can be very subtle and evaluation of abnormal elbow fat pads is critical and often the only diagnostic clue
- Type 2- displaced by 2-mm or > with rotational block
- Type 3- comminuted >2-3 fragments and
- Type4 is presented with RH fx, posterior elbow dislocation and sometimes Coronoid process fracture often d/t Brachialis M avulsion
Rx : Type 1 managed non-operatively by immobilization and movement rehab. Type 2- ORIF if rotational block. Type 3 and 4, ORIF and RH resection or RH arthroplasty
- Note abnormally displaced anterior fat pad (orange arrow) and the emergence of the posterior fat pad (green arrow) that is usually deep in the olecranon fossa and not seen unless acute hemarthrosis or other effusiondevelopsFat pad signs are most reliable indicators of intra-articular elbow Fx
- Mason type 1 RH Fx can be v. subtle and missed. Radiographic search should involve a
close evaluation of positive fat pad signs. Note anterior fat pad displacement aka Sail sign and the presence of the post fat pad d/t acute bleed

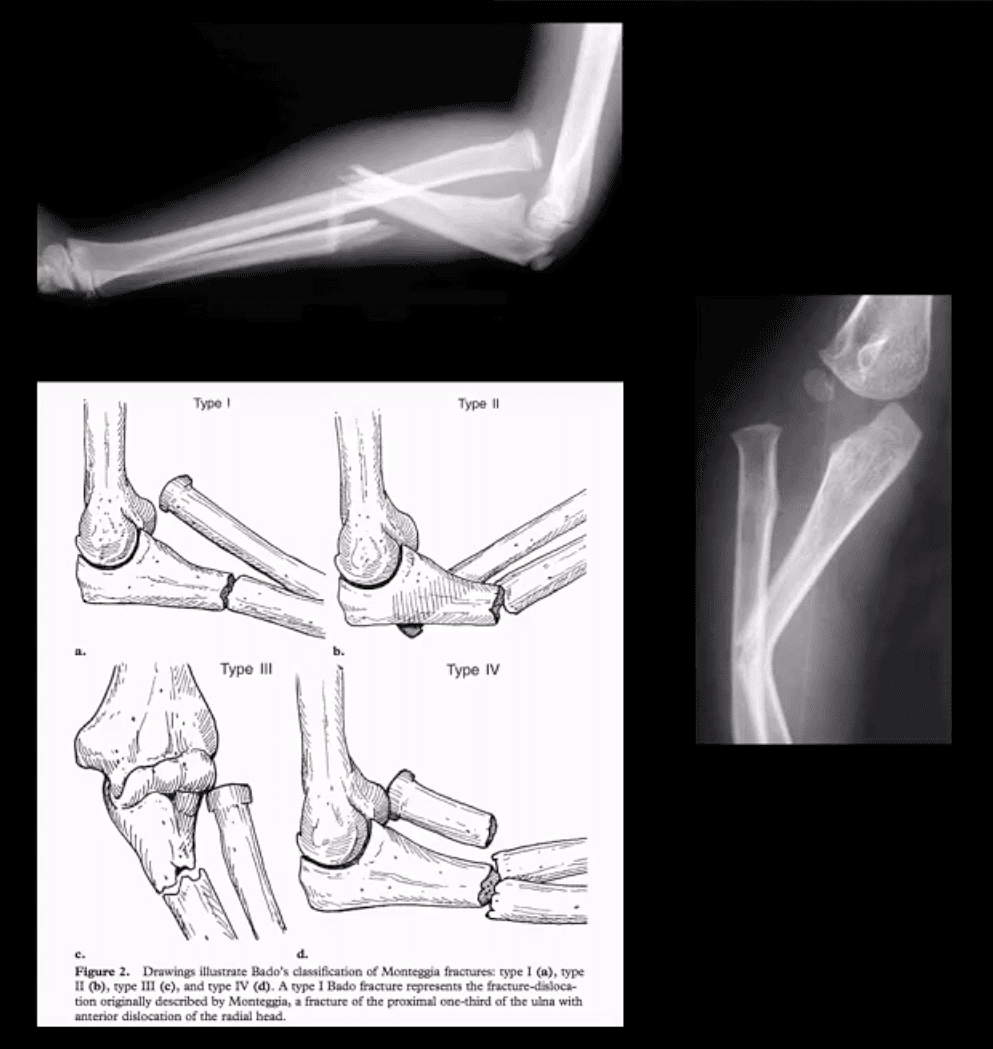
- Monteggia fracture-dislocations: prox 1/3ulnar shaft Fx. with concomitant dislocation of PRUJ (radial head). FOOSH injury. Children4-12 y.o. Infrequent in adults.
- X-rays readily reveal ulnar Fx but radial head dislocation may be subtle and occasionally missed. This is a serious injury leading to elbow disability if Dx delayed 2-3 weeks or left untreated. X-rays are typically sufficient:Rx: casting vs. operative.
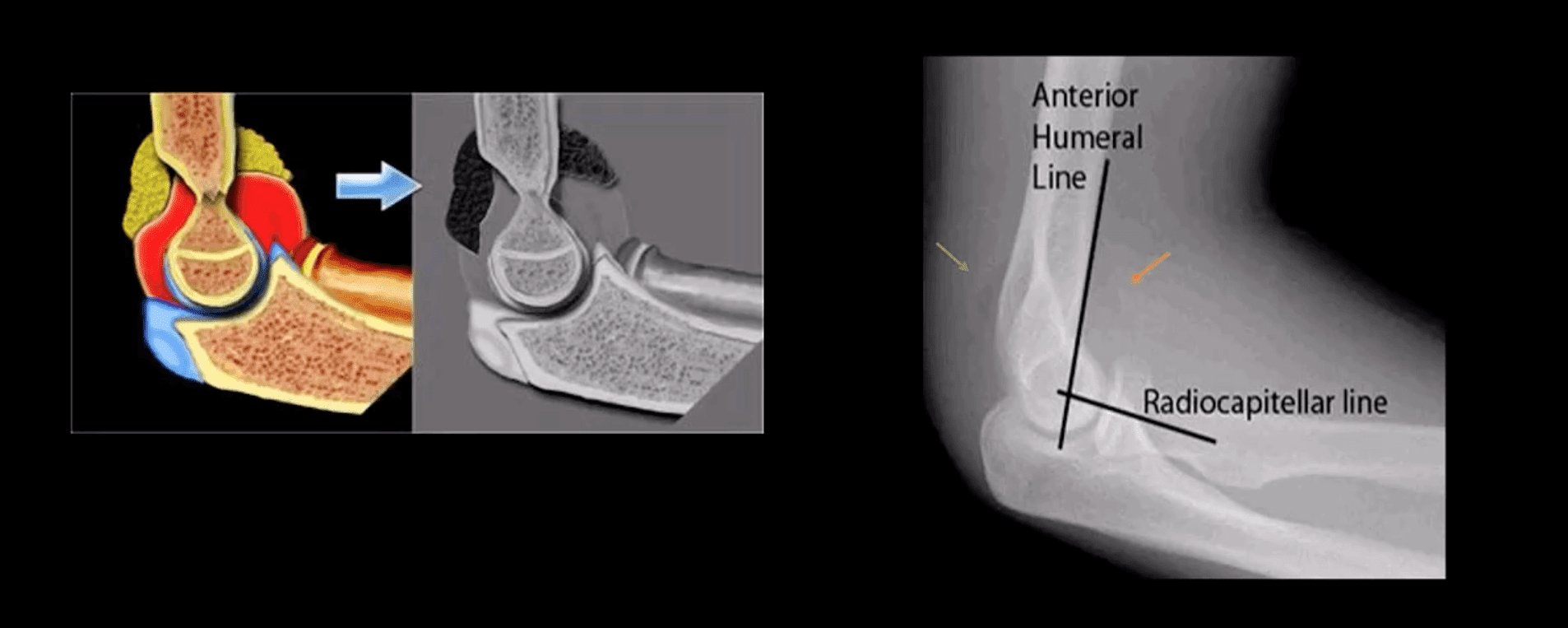
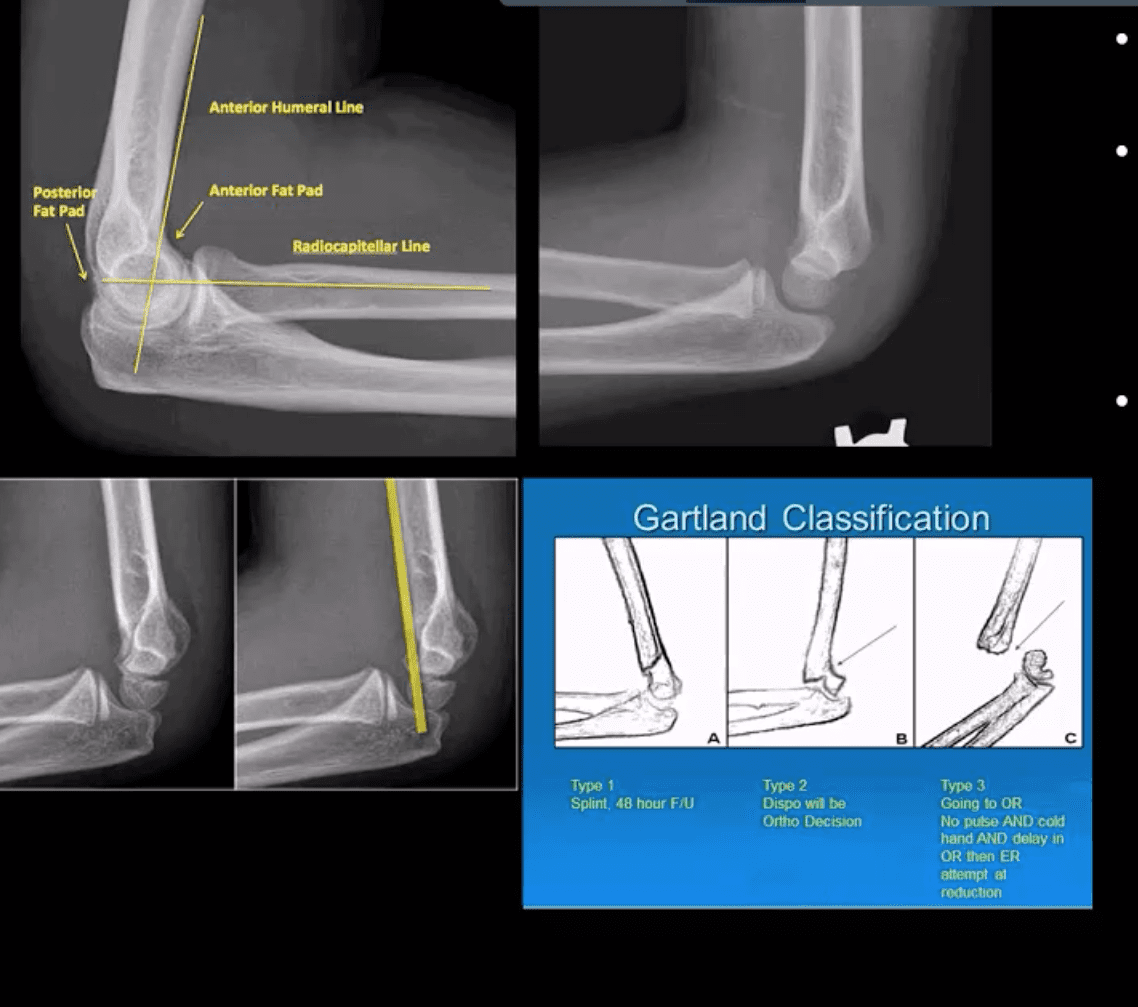
- Supracondylar Fx: this is the M/C elbow Fx in children.
- Especially, the un-displaced types 1(top right) is difficult to Dx. Abnormality of “fat pads” and anterior humeral line and radiocapitella line disturbance are often most reliable
- Type 3 carries a particularly high risk for Volkmann contracture (vascularischemic-necrosis of the anterior forearm muscle compartment
Elbow complaints in a young athlete
- Epicondyle Fx: common pediatric injury, about 10%.Essentially an avulsion Fx and a MUCL tear. Medial epicondyle is m/c Fx. FOOSH is the m/c mechanism.M>F. If minimally displaced or undisplaced can be treated with casting esp. in non-dominant arm. If displaced as in this case, require ORIF.
- Medial epicondyle avulsive Fx in a young baseball pitcher was coined a “little league elbow” in the 60sand now should be avoided to avoid confusion
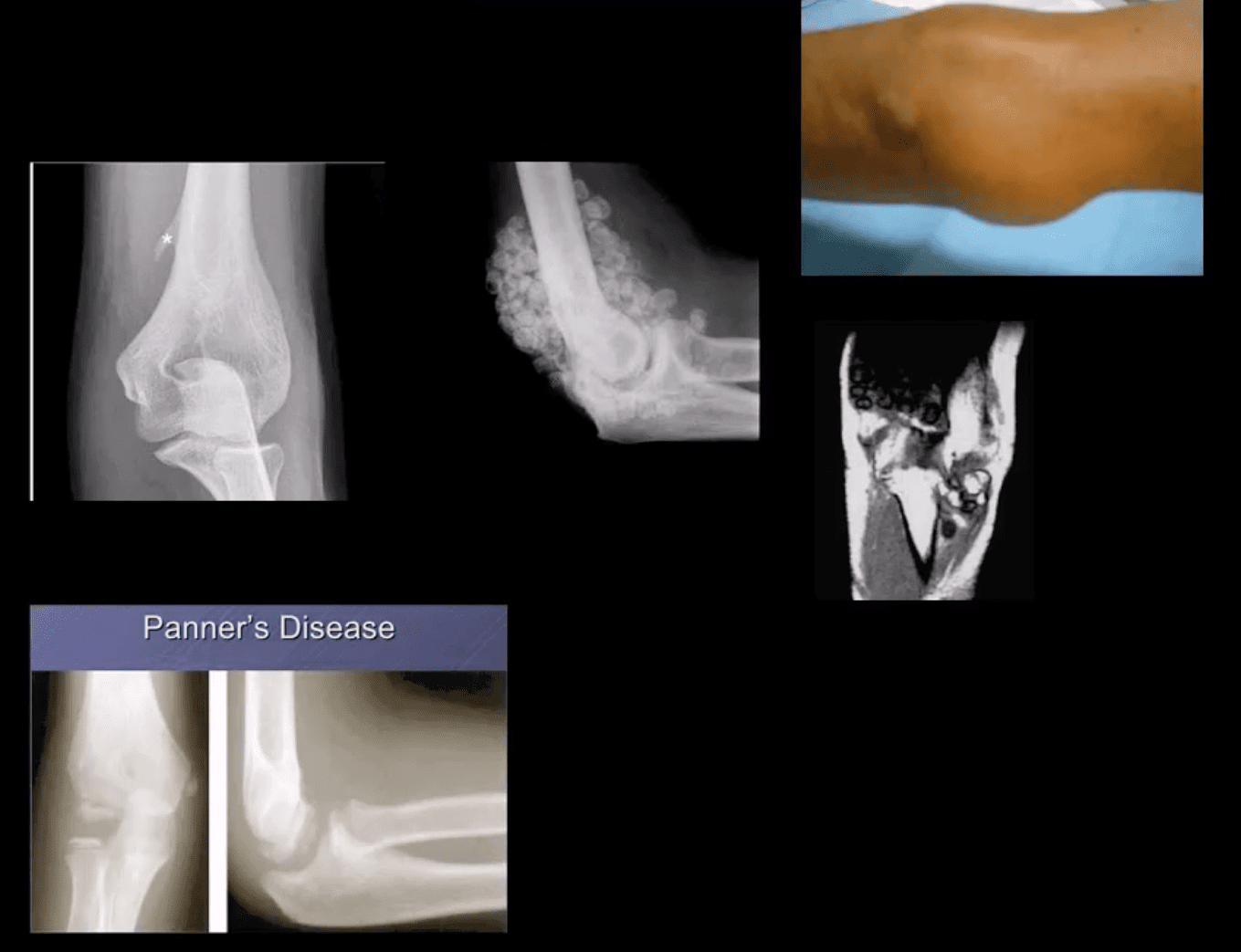
- OCD of the Capitellum is a common athletic injury induced by repeated compression/flexion. OCD must be DDx from Panner’s disease or osteochondritis typically presented in younger patients
- Difficulty in diagnosis may stem from multipleapophysis about the elbow (see CRITOE)
- Imaging: 1st step: x-rays followed by MRI and/or MRarthrogramme if indicated.
- CT may help with complex injury evaluation. MRI and/or MSKUS may help with a
ligament injury.
Elbow Arthritis
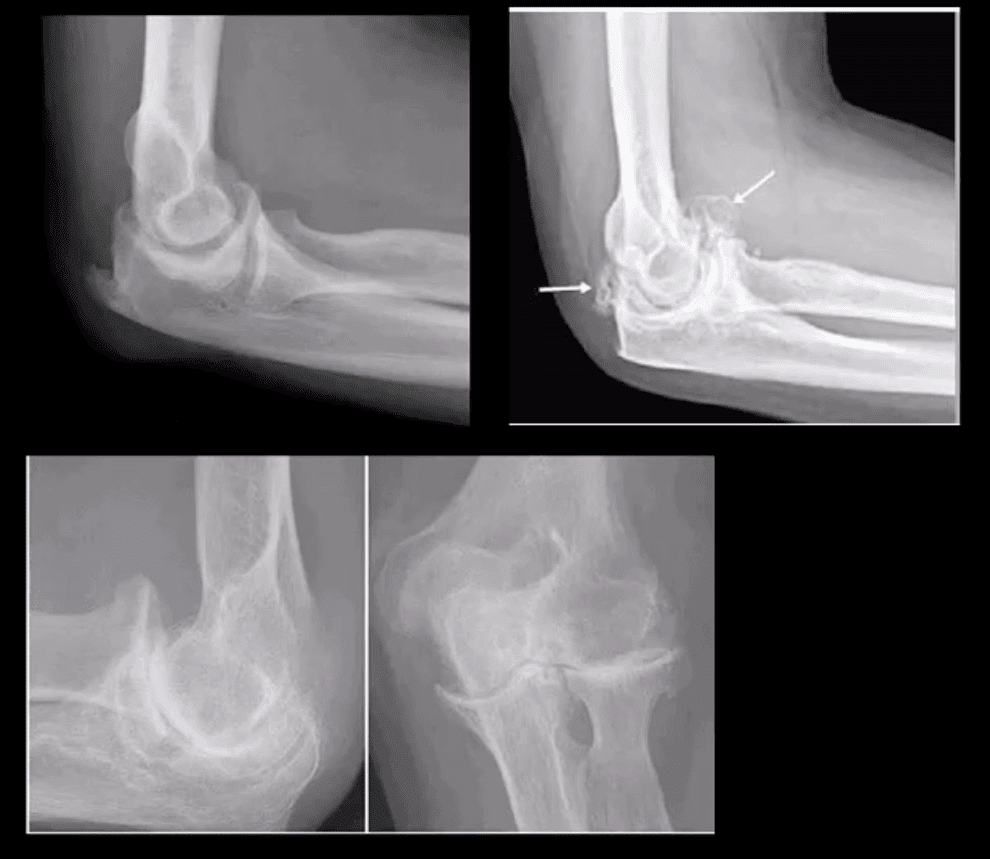
- DJD of the elbow is uncommon and typically 2nd to trauma, occupation, CPPD, OCD of theCapitellum or other pathology. Clinically: pain, reduced ROM esp. in dominant arm, deterioration of ADL. Loss of terminal flexion and extension. 50% develop Ulnarcompressive neuropathy. Rx: conservative,arthroscopic debridement/osteophytes removal, capsular release. In older patients and not active patients Total Elbow Arthroplasty (TEA) can be used
- Imaging: x-radiography is sufficient, CT helps with pre-operative planning
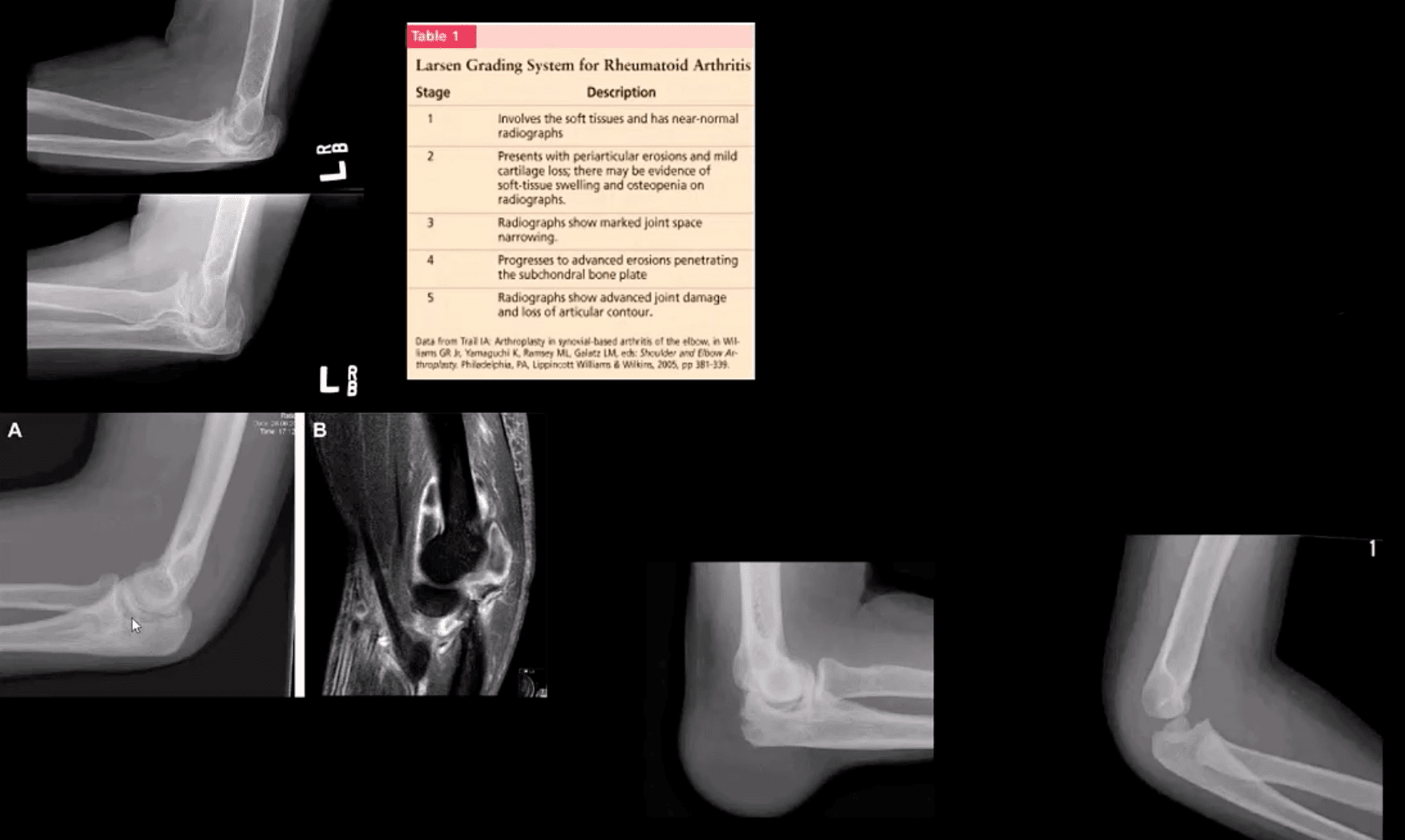
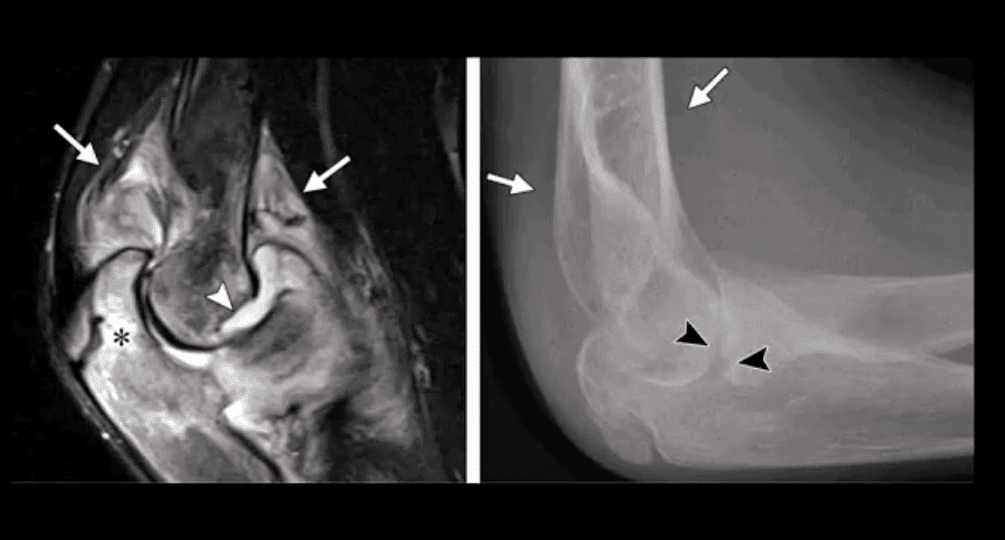
- Inflammatory Arthritis: RA of the elbow is frequent (20-50%) and destructive d/t synovitis, pannus, bone/cartilage, and ligamentous destruction/laxity. Clinically: begins after the onset of hands symptoms with, symmetrical swelling, pain, reduced ROM, flexion contracture. Presence of rheumatoid nodules can be noted along the olecranon and posterior forearm. Rx: DMARD, operative tendons repair.
- Imaging: x-radiography with early non-specific effusion (fat pads),later: erosions, symmetric JSL, osteopenia. MSK US helps early Dx. MRI reveals synovitis, bone edema correlates with pre-erosive x-ray findings, synovial enhancement on FS T1+C.
- Gouty Arthritis: may affect the elbow but less than in the lower extremity. Olecranon bursitis causing a “rising sun sign” on x-rays with or w/o bone erosions. Aspiration and polarised microscopy revealing needle-shaped negatively birefringent monosodium urate crystals. Rx: colchicine, other meds.
- Septic Arthritis: consider in diabetics, IV drug users, concurrent RA, patients with active TB, gonococcal in young adults. Clinically presents as monoarthritis with or w/o constitutional signs. X-ray: poor detection in early stages. US may show effusion and high Doppler.MRI: effusion, osseous edema. Bone scintigraphy can help as well. Labs: CBC, ESR, CRP. Diagnostic arthrocentesis with gram staining and culture are crucial. Rx: Prompt IV antibiotics
- Juvenile Idiopathic Arthritis (JIA) considered M/C chronic disease of childhood and precedes IBD infrequency. Dx is clinical and imaging: Criteria: Joint pain and swelling in a child 0-16-years for 6-weeks or longer. Many forms exist M/C pauciarticular(oligoarticular) 40%, F>M, associated with ocular involvement (iridocyclitis) and potential blindness. Polyarticular and Systemic forms.
- Elbow is frequently affected along with the knee, wrists, and hands, especially in polyarticular dz.
- Labs: ESR/CRP RF-VE in most cases
- Imaging: early x-ray features are non-specific. Later: osseous erosion, destruction of joint cartilage, overgrowth of articular epiphyses, early closure of physis. Delayed features: 2nd DJD, joint ankyloses.DDx: hemophilic arthropathy. Cervical radiographs are crucial.
- Rx: DMARD, conservative care
Miscellaneous pathologies
- Supracondylar process: 2% of the population. Described by Sir JohnStruthers in 1854. Fibrous band(Ligament of Struthers) may lead to compression of the Median N. DDx fromOsteochondroma that typically points away from the joint
- Primary synovial chondrometaplasia (Reichel Syndrome): abnormalmetaplasia of synovial cells shedding cartilage into joint potentially causing DJD, extrinsic bone erosion, synovitis, nerve compressions etc. Removedoperatively. Imaging: multiple osseocartilaginous loose bodies of relatively equal sizes in the joint cavityDDx with DJD and 2ndosteochondromatosis. MRI-low signal onT1 and T2 with potential joint effusion. Ina tight joint like the elbow may present with large joint distention.•
- Panner’s Disease: osteochondrosis of theCapitellum typically in 5-10 y.o. young athlete DDX from OCD of Capitellum(discussed) that occurs in teenagers.Clinically: pain on activity. Recovery occurs in most cases by spontaneous healing. Imaging: x-rays reveal sclerosis and slight fragmentation of theCapitellum w/o loose body. MRI: low T1and high T2 signal in the entireCapitellum.
- Myositis Ossificance:
Soft Tissue & Bone Neoplasms about the Elbow
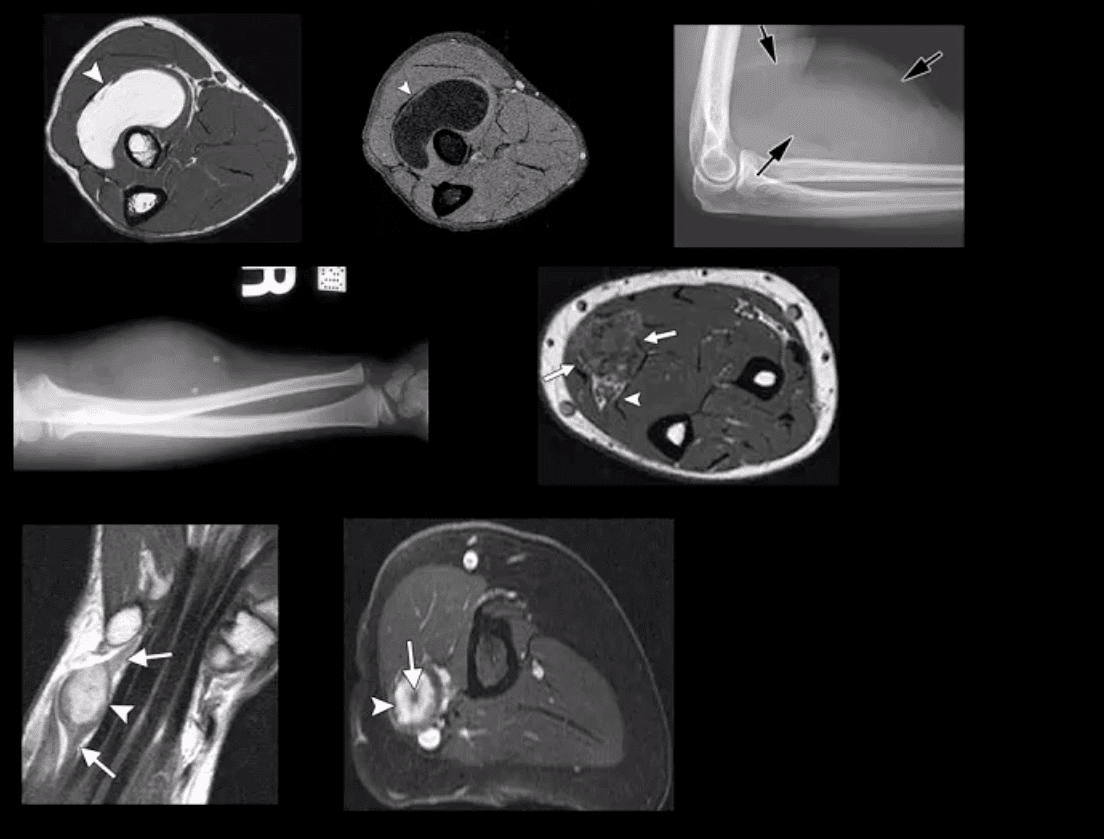
- Lipoma: intramuscular, subcutaneous. Most common soft tissue neoplasms. Composed of fat but a substantial number may undergo fat necrosis-calcification-fibrosis. Typically remains benign. Occasionally difficult to DDx from a well-differentiated liposarcoma. Imaging: x radiography: radiolucent lesion well-circumscribed with or w/o calcification. US and MRI are important. On MRIT1high, T2 low SI.
- Hemangioma: benign vascular lesion, often composed of multiple vascular channels. Capillary vs. cavernous. More common in children, but found in any age. May often form phleboliths (calcification). Imaging: x-rays reveal soft tissue mass containing phleboliths. MRI: T1-high or variable signal. T2-high signal in areas of slow flow. “bag of worms” sign. Biopsy best avoided. Rx: difficult: local excision vs. embolization vs. observation. High recurrence.
- Peripheral Nerve sheath tumor (PNST): benign vs.malignant. Greater incidence in NF1 with a higher risk of malignant PNST. Benign PNST: Schwannoma vs.Neurofibroma. Spinal vs. peripheral nerves. Histology: Schwann cells interspersed with fibroblast and vessels.Clinically: pts in 20s and 30s, palpable mass with or w/o local pressure. Imaging: MRI: T1: split-fat sign, T2: target sign. T1+C enhancement
- Soft Tissue Sarcomas: MFH, Synovial sarcoma,(discussed), Liposarcoma (more frequent in the retroperitoneum) Dx: MRI. Clinically: Dx is delayed d/t painless enlarging mass often ignored. Clinically palpable mass deserves MRI examination, US may be helpful. Biopsy confirms Dx.
- Malignant bone Neoplasms: Children: OSA, Ewing’s sarcoma (discussed) Adults: Mets, Myeloma (discussed)
The Elbow
Post Disclaimer
Professional Scope of Practice *
The information herein on "The Elbow: Diagnostic Imaging Approach | El Paso, TX." is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Our information scope is limited to Chiropractic, musculoskeletal, physical medicines, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somatovisceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and/or functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and directly or indirectly support our clinical scope of practice.*
Our office has reasonably attempted to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez, DC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, RN*, CCST, IFMCP*, CIFM*, ATN*
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807, New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Florida
Florida License RN License # RN9617241 (Control No. 3558029)
License Compact Status: Multi-State License: Authorized to Practice in 40 States*
Presently Matriculated: ICHS: MSN* FNP (Family Nurse Practitioner Program)
Dr. Alex Jimenez DC, MSACP, RN* CIFM*, IFMCP*, ATN*, CCST
My Digital Business Card