


These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Table of Contents
Clinical Application of Neuromuscular Techniques: Tensor Fascia Lata
Assessment of shortness in tensor fascia lata (TFL)
The test recommended is a modified form of Ober’s test (see Fig. 4.14).
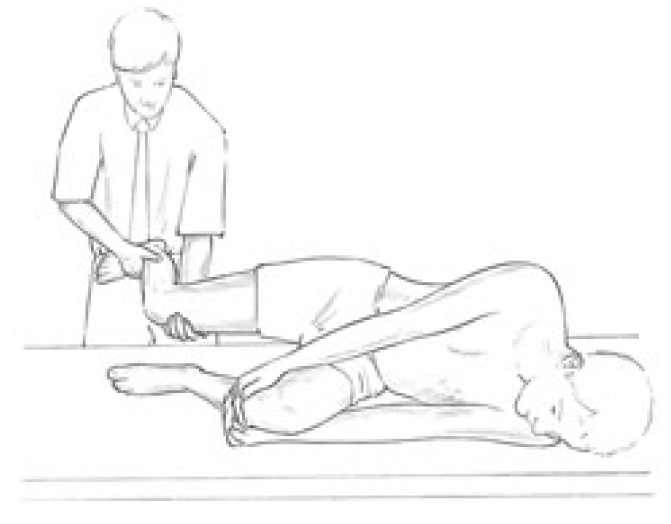
Figure 4.14 Assessment for shortness of TFL – modified Ober’s test. When the hand supporting the flexed knee is removed the thigh should fall to the table if TFL is not short.
Patient is side-lying with back close to the edge of the table. The practitioner stands behind the patient, whose lower leg is flexed at hip and knee and held in this position, by the patient, for stability. The tested leg is supported by the practitioner, who must ensure that there is no hip flexion, which would nullify the test.
The leg is extended only to the point where the iliotibial band lies over the greater trochanter. The tested leg is held by the practitioner at ankle and knee, with the whole leg in its anatomical position, neither abducted nor adducted and not forward or backward of the body.
Box 4.5 Notes on TFL
- Mennell (1964) and Liebenson (1996) say that TFL shortness can produce all the symptoms of acute and chronic sacroiliac problems.
- Pain from TFL shortness can be localised to the posterior superior iliac spine (PSIS), radiating to the groin or down any aspect of the thigh to the knee.
- Although the pain may arise in the sacroiliac (SI) joint, dysfunction in the joint may be caused and maintained by taut TFL structures.
- Pain from the band itself can be felt in the lateral thigh, with referral to hip or knee.
- TFL can be ‘riddled’ with sensitive fibrotic deposits and trigger point activity.
- There is commonly a posteriority of the ilium associated with short TFL.
- TFL’s prime phasic activity (all postural structures also have some phasic function) is to assist the gluteals in abduction of the thigh.
- If TFL and psoas are short they may, according to Janda, ‘dominate’ the gluteals on abduction of the thigh, so that a degree of lateral rotation and flexion of the hip will be produced, rotating the pelvis backwards.
- Rolf (1977) points out that persistent exercise such as cycling will shorten and toughen the fascial iliotibial band ‘until it becomes reminiscent of a steel cable’. This band crosses both hip and knee, and spatial compression allows it to squeeze and compress cartilaginous elements such as the menisci. Ultimately, it will no longer be able to compress, and rotational displacement at knee and hip will take place.
The practitioner carefully introduces flexion at the knee to 90°, without allowing the hip to flex, and then, holding just the ankle, allows the knee to fall towards the table. If TFL is normal, the thigh and knee will fall easily, with the knee contacting the table surface (unless unusual hip width, or thigh length prevent this).
If the upper leg remains aloft, with little sign of ‘falling’ towards the table, then either the patient is not letting go or the TFL is short and does not allow it to fall. As a rule the band will palpate as tender under such conditions.
Lewit’s TFL Palpation
(Lewit 1999; see also functional assessment method in Ch. 5)
Patient is side-lying and practitioner stands facing the patient’s front, at hip level. The practitioner’s cephalad hand rests over the anterior superior iliac spine (ASIS) so that it can also palpate over the trochanter. It should be placed so that the fingers rest on the TFL and trochanter with the thumb on gluteus medius. The caudad hand rests on the mid-thigh to apply slight resistance to the patient’s effort to abduct the leg.
The patient’s table-side leg is slightly flexed to provide stability, and there should be a vertical line to the table between one ASIS and the other (i.e. no forwards or backwards ‘roll’ of the pelvis). The patient abducts the upper leg (which should be extended at the knee and slightly hyperextended at the hip) and the practitioner should feel the trochanter ‘slip away’ as this is done.
If, however, the whole pelvis is felt to move rather than just the trochanter, there is inappropriate muscular imbalance. (In balanced abduction gluteus comes into action at the beginning of the movement, with TFL operating later in the pure abduction of the leg. If there is an overactivity (and therefore shortness) of TFL, then there will be pelvic movement on the abduction, and TFL will be felt to come into play before gluteus.)
The abduction of the thigh movement will then be modified to include external rotation and flexion of the thigh (Janda 1996). This confirms a stressed postural structure (TFL), which implies shortness.
It is possible to increase the number of palpation elements involved by having the cephalad hand also palpate (with an extended small finger) quadratus lumborum during leg abduction. In a balanced muscular effort to lift the leg sideways, quadratus should not become active until the leg has been abducted to around 25–30°. When quadratus is overactive it will often start the abduction along with TFL, thus producing a pelvic tilt. (See also Fig. 5.11A and B)
Method (a) Supine MET treatment of shortened TFL (Fig. 4.15) The patient lies supine with the unaffected leg flexed at hip and knee. The affected side leg is adducted to its barrier which necessitates it being brought under the opposite leg/foot.

Figure 4.15 MET treatment of TFL (see Fig. 1.4 for description of isolytic variation). If a standard MET method is being used, the stretch will follow the isometric contraction in which the patient will attempt to move the right leg to the right against sustained resistance. It is important for the practitioner to maintain stability of the pelvis during the procedure. Note: the hand positions in this figure are a variation of those described in the text.
Using guidelines for acute and chronic problems, the structure will either be treated at, or short of, the barrier of resistance, using light or fairly strong isometric contractions for short (7 second) or long (up to 20 seconds) durations, using appropriate breathing patterns as described earlier in this chapter (Box 4.2).
The practitioner uses his trunk to stabilise the patient’s pelvis by leaning against the flexed (nonaffected side) knee. The practitioner’s caudad arm supports the affected leg so that the knee is stabilised by the hand. The other hand maintains a stabilising contact on the affected side ASIS.
The patient is asked to abduct the leg against resistance using minimal force. After the contraction ceases and the patient has relaxed using appropriate breathing patterns, the leg is taken to or through the new restriction barrier (into adduction past the barrier) to stretch the muscular fibres of TFL (the upper third of the structure).
Care should be taken to ensure that the pelvis is not tilted during the stretch. Stability is achieved by the practitioner increasing pressure against the flexed knee/thigh. This whole process is repeated until no further gain is possible.
Method (b) Alternative supine MET treatment of shortened TFL (Fig. 4.16) The patient adopts the same position as for psoas assessment, lying at the end of the table with non-tested side leg in full hip flexion and held by the patient, with the tested leg hanging freely, knee flexed.

Figure 4.16 MET treatment of psoas using Grieve’s method, in which there is placement of the patient’s foot, inverted, against the operator’s thigh. This allows a more precise focus of contraction into psoas when the hip is flexed against resistance.
The practitioner stands at the end of the table facing the patient so that his left lower leg (for a right-sided TFL treatment) can contact the patient’s foot. The practitioner’s left hand is placed on the patient’s distal femur and with this he introduces internal rotation of the thigh, and external rotation of the tibia (by means of light pressure on the distal foot from his lower leg).
During this process the practitioner senses for resistance (the movement should have an easy ‘springy’ feel, not wooden or harsh) and observes for a characteristic depression or groove on the lateral thigh, indicating shortness of TFL.
This resistance barrier is identified and the leg held just short of it for a chronic problem, as the patient is asked to externally rotate the tibia, and to adduct the femur, against resistance, for 7–10 seconds. Following this the practitioner eases the leg into a greater degree of internal hip rotation and external tibial rotation, and holds this stretch for 10–30 seconds.
Method (c) Isolytic variation If an isolytic contraction is introduced in order to stretch actively the interface between elastic and non-elastic tissues, then there is a need to stabilise the pelvis more efficiently, either by use of wide straps or another pair of hands holding the ASIS downwards towards the table during the stretch.
The procedure consists of the patient attempting to abduct the leg as the practitioner overcomes the muscular effort, forcing the leg into adduction. The contraction/stretch should be rapid (2–3 seconds at most to complete). Repeat several times.
Method (d) Side-lying MET treatment of TFL The patient lies on the affected TFL side with the upper leg flexed at hip and knee and resting forward of the affected leg. The practitioner stands behind patient and uses caudad hand and arm to raise the affected leg (which is on the table) while stabilising the pelvis with the cephalad hand, or uses both hands to raise the affected leg into slight adduction (appropriate if strapping used to hold pelvis to table).
The patient contracts the muscle against resistance by trying to take the leg into abduction (towards the table) using breathing assistance as appropriate (see notes on breathing, Box 4.2). After the effort, on an exhalation, the practitioner lifts the leg into adduction beyond the barrier to stretch the interface between elastic and non-elastic tissues. Repeat as appropriate or modify to use as an isolytic contraction by stretching the structure past the barrier during the contraction.
Additional TFL Methods
Mennell has described superb soft tissue stretching techniques for releasing TFL. These involve a series of snapping actions applied by thumbs to the anterior fibres with patient side-lying, followed by a series of heel of hand thrusts across the long axis of the posterior TFL fibres.
Additional release of TFL contractions is possible by use of elbow or heel of hand ‘stripping’ of the structure, neuromuscular deep tissue approaches (using thumb or a rubber-tipped T-bar) applied to the upper fibres and those around the knee, and specific deep tissue release methods. Most of these are distinctly uncomfortable and all require expert tuition.
Self-Treatment and Maintenance
The patient lies on her side, on a bed or table, with the affected leg uppermost and hanging over the edge (lower leg comfortably flexed). The patient may then introduce an isometric contraction by slightly lifting the hanging leg a few centimeters, and holding this position for 10 seconds, before slowly releasing and allowing gravity to take the leg towards the floor, so introducing a greater degree of stretch.
This is held for up to 30 seconds and the process is then repeated several times in order to achieve the maximum available stretch in the tight soft tissues. The counterforce in this isometric exercise is gravity.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez

Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.

WELLNESS TOPIC: EXTRA EXTRA: Managing Workplace Stress
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card
Comments are closed.