


Table of Contents
What is a Herniated Disc?
The spine is made up of 24 bones, called vertebrae, which are stacked on top of one another. These spinal bones are ultimately connected, creating a canal to protect the spinal cord. In between each vertebra are fluid-filled intervertebral discs which act as shock absorbers for the spine. Over time, however, these flexible, jelly donut-like discs can begin to herniate, where the nucleus of the intervertebral disc pushes against its outer ring, causing low back pain. Below, we will demonstrate the various types of herniated discs and discuss their causes, symptoms and treatment options.
Abstract
Background Context
The paper ‘‘Nomenclature and classification of lumbar disc pathology, recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology,’’ was published in 2001 in Spine (© Lippincott, Williams & Wilkins). It was authored by David Fardon, MD, and Pierre Milette, MD, and formally endorsed by the American Society of Spine Radiology (ASSR), American Society of Neuroradiology (ASNR), and North American Spine Society (NASS). Its purpose was to promote greater clarity and consistency of usage of spinal terminology, and it has served this purpose well for over a decade. Since 2001, there has been sufficient evolution in our understanding of the lumbar disc to suggest the need for revision and updating of the original document. The revised document is presented here, and it represents the consensus recommendations of contemporary combined task forces of the ASSR, ASNR, and NASS. This article reflects changes consistent with current concepts in radiologic and clinical care.
Purpose
To provide a resource that promotes a clear understanding of lumbar disc terminology amongst clinicians, radiologists, and researchers. All the concerned need standard terms for the normal and pathologic conditions of lumbar discs that can be used accurately and consistently and thus best serve patients with disc disorders.
Study Design
This article comprises a review of the literature.
Methods
A PubMed search was performed for literature pertaining to the lumbar disc. The task force members individually and collectively reviewed the literature and revised the 2001 document. The revised document was then submitted for review to the governing boards of the ASSR, ASNR, and NASS. After further revision based on the feedback from the governing boards, the article was approved for publication by the governing boards of the three societies, as representative of the consensus recommendations of the societies.
Results
The article provides a discussion of the recommended diagnostic categories pertaining to the lumbar disc: normal; congenital/developmental variation; degeneration; trauma; infection/inflammation; neoplasia; and/or morphologic variant of uncertain significance. The article provides a glossary of terms pertaining to the lumbar disc, a detailed discussion of these terms, and their recommended usage. Terms are described as preferred, nonpreferred, nonstandard, and colloquial. Updated illustrations pictorially portray certain key terms. Literature references that provided the basis for the task force recommendations are included.
Conclusions
We have revised and updated a document that, since 2001, has provided a widely
Keywords
Annular fissure, Annular tear, Disc bulge (bulging disc), Disc degeneration, Disc extrusion, Disc herniation, Disc nomenclature, Disc protrusion, High-intensity zone, Lumbar intervertebral disc
Preface
The nomenclature and classification of lumbar disc pathology consensus, published in 2001, by the collaborative efforts of the North American Spine Society (NASS), the American Society of Spine Radiology (ASSR) and the American Society of Neuroradiology (ASNR), has guided radiologists, clinicians, and interested public for over a decade [1]. This document has passed the test of time. Responding to an initiative from the ASSR, a task force of spine physicians from the ASSR, ASNR, and NASS has reviewed and modified the document. This revised document preserves the format and most of the language of the original, with changes consistent with current concepts in radiologic and clinical care. The modifications deal primarily with the following: updating and expansion of Text, Glossary, and References to meet contemporary needs; revision of Figures to provide greater clarity; emphasis of the term ‘‘annular fissure’’ in place of ‘‘annular tear’’; refinement of the definitions of ‘‘acute’’ and ‘‘chronic’’ disc herniations; revision of the distinction between disc herniation and asymmetrically bulging disc; elimination of the Tables in favor of greater clarity from the revised Text and Figures; and deletion of the section of Reporting and Coding because of frequent changes in those practices, which are best addressed by other publications. Several other minor amendments have been made. This revision will update a workable standard nomenclature, accepted and used universally by imaging and clinical physicians.
Introduction and History
Physicians need standard terms for normal and pathologic conditions of lumbar discs [2, 3, 4, 5]. Terms that can be interpreted accurately, consistently, and with reasonable precision are particularly important for communicating impressions gained from imaging for clinical diagnostic and therapeutic decision-making. Although
In 1995, a multidisciplinary task force from the NASS addressed the deficiencies in commonly used terms defining the conditions of the lumbar disc. It cited several documentations of the problem [6, 7, 8, 9, 10, 11] and made detailed recommendations for standardization. Its work was published in a copublication of the NASS and the American Academy of Orthopaedic Surgeons [9]. The work had not been otherwise endorsed by major organizations and had not been recognized as authoritative by radiology organizations. Many previous [3, 7, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19] and some subsequent [20, 21, 22, 23, 24, 25] efforts addressed the issues, but were of more limited scope and none had gained a widespread acceptance.
Although the NASS 1995 effort was the most comprehensive at the time, it remained deficient in clarifying some controversial topics, lacking in its treatment of some issues, and did not provide recommendations for standardization of classification and reporting. To address the remaining needs, and in hopes of securing endorsement sufficient to result in universal standardizations, joint task forces (Co-Chairs David Fardon, MD, and Pierre Milette, MD) were formed by the NASS, ASNR, and ASSR, resulting in the first version of the document ‘‘Nomenclature and classification of lumbar disc pathology’’ [1]. Since then, time and experience suggested the need for revisions and updating of the original document. The revised document is presented here.
The general principles that guided the original document remain unchanged in this revision. The definitions are based on the anatomy and pathology, primarily as visualized on imaging studies. Recognizing that some criteria, under some circumstances, may be unknowable to the observer, the definitions of the terms are not dependent on or imply the value of specific tests. The definitions of diagnoses are not intended to imply external etiologic events such as trauma, they do not imply relationship to symptoms, and they do not define or imply the need for specific treatment.
The task forces, both current and former, worked from a model that could be expanded from a primary purpose of providing understanding of reports of imaging studies. The result provides a simple classification of diagnostic terms, which can be expanded, without contradiction, into more precise subclassifications. When reporting pathology, degrees of uncertainty would be labeled as such rather than compromising the definitions of the terms.
All terms used in the classifications and subclassifications are defined and those definitions are adhered to throughout the model. For a practical purpose, some existing English terms are given meanings different from those found in some contemporary dictionaries. The task forces provide a list and classification of the recommended terms, but, recognizing the nature of language practices, discuss and include in the Glossary, commonly used and misused nonrecommended terms and nonstandard definitions.
Although the principles and most of the definitions of this document can be easily extrapolated to the cervical and dorsal spine, the focus is on the lumbar spine. Although clarification of terms related to posterior elements, dimensions of the spinal canal, and status of neural tissues is needed, this work is limited to the discussion of the disc. While it is not always possible to discuss fully the definition of anatomical and pathologic terms without some reference to symptoms and etiology, the definitions themselves stand the test of independence from etiology, symptoms, or treatment. Because of the focus on anatomy and pathology, this work does not define certain clinical syndromes that may be related to lumbar disc pathology [26].
Guided by those principles, we have revised and updated a document that, since 2001, has provided a widely acceptable nomenclature that is workable for all forms of observation, that addresses contour, content, integrity, organization, and spatial relationships of the lumbar disc; and that serves a system of classification and reporting built upon that nomenclature.
Diagnostic Category & Subcategory Recommendations
These recommendations present diagnostic categories and subcategories intended for classification and reporting of imaging studies. The terminology used throughout these recommended categories and subcategories remains consistent with detailed explanations given in the Discussion and with the preferred definitions presented in the Glossary.
The diagnostic categories are based on pathology. Each lumbar disc can be classified in terms of one, and occasionally more than one, of the following diagnostic categories: normal; congenital/developmental variation; degeneration; trauma; infection/inflammation; neoplasia; and/or morphologic variant of uncertain significance. Each diagnostic category can be subcategorized to various degrees of specificity according to the information available and purpose to be served. The data available for categorization may lead the reporter to characterize the interpretation as ‘‘possible,’’ ‘‘probable,’’ or ‘‘definite.’’
Note that some terms and definitions discussed below are not recommended as preferred terminology, but are included to facilitate the interpretation of vernacular and, in some cases, improper use. Terms may be defined as preferred, nonpreferred, or nonstandard. Nonstandard terms by consensus of the organizational task forces should not be used in the manner described.
Normal
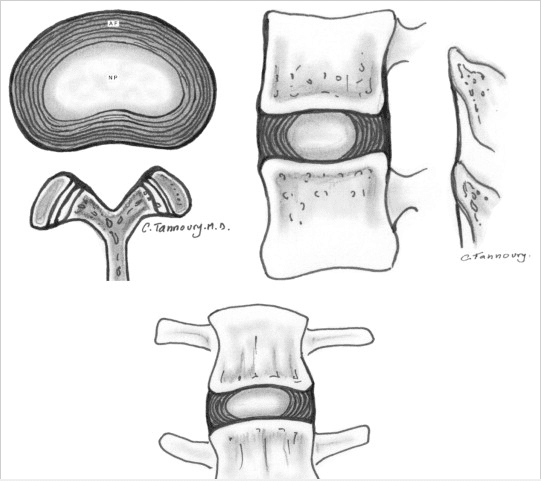
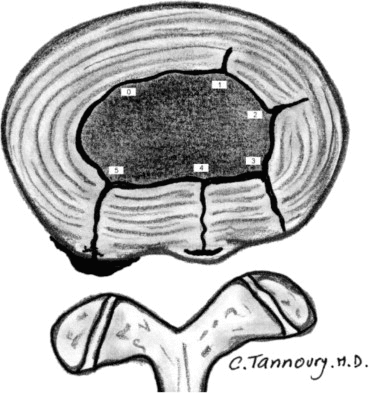
Normal defines discs that are morphologically normal, without the consideration of the clinical context and not inclusive of degenerative, developmental, or adaptive changes that could, in some contexts (eg, normal aging, scoliosis, spondylolisthesis), be considered clinically normal (Fig. 1).
Congenital/Developmental Variation
The congenital/developmental variation category includes discs that are congenitally abnormal or that have undergone changes in their morphology as an adaptation of abnormal growth of the spine, such as from scoliosis or spondylolisthesis.
Degeneration
Degenerative changes in the discs are included in a broad category that includes the subcategories annular fissure, degeneration, and herniation.
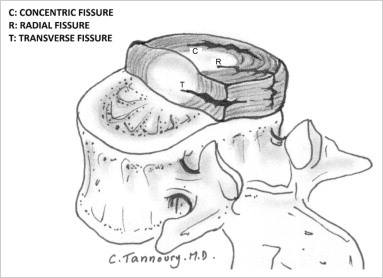
Annular fissures are separations between the annular fibers or separations of annular fibers from their attachments to the vertebral bone. Fissures are sometimes classified by their orientation. A ‘‘concentric fissure’’ is a separation or delamination of annular fibers parallel to the peripheral contour of the disc (Fig. 2). A ‘‘radial fissure’’ is a vertically, horizontally, or obliquely oriented separation of (or rent in) annular fibers that extends from the nucleus peripherally to or through the annulus. A ‘‘transverse fissure’’ is a horizontally oriented radial fissure, but the term is sometimes used in a narrower sense to refer to a horizontally oriented fissure limited to the peripheral annulus that may include separation of annular fibers from the apophyseal bone. Relatively wide annular fissures, with stretch of the residual annular margin, at times including avulsion of an annular fragment, have sometimes been called ‘‘annular gaps,’’ a term that is relatively new and not accepted as standard [27]. The term ‘‘fissures’’ describes the spectrum of these lesions and does not imply that the lesion is a consequence of injury.
Use of the term ‘‘tear’’ can be misunderstood because the analogy to other tears has a connotation of injury, which is inappropriate in this context. The term ‘‘fissure’’ is the correct term. Use of the term ‘‘tear’’ should be discouraged and, when it appears, should be recognized that it is usually meant to be synonymous with ‘‘fissure’’ and not reflective of the result of injury. The original version of this document stated preference for the term ‘‘fissure’’ but regarded the two terms as almost synonymous. However, in this revision, we regard the term ‘‘tear’’ as nonstandard usage.
Degeneration may include any or all of the following: desiccation, fibrosis, narrowing of the disc space, diffuse bulging of the annulus beyond the disc space, fissuring (ie, annular fissures), mucinous degeneration of the annulus, intradiscal gas [28], osteophytes of the vertebral apophyses, defects, inflammatory changes, and sclerosis of the end plates [15, 29, 30, 31, 32, 33, 34].
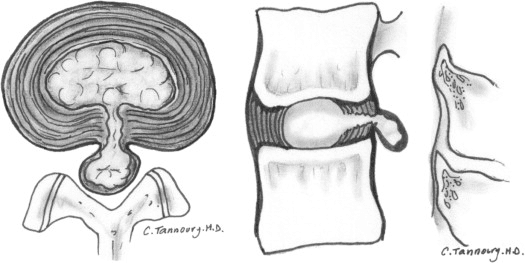
Herniation is broadly defined as a localized or focal displacement of disc material beyond the limits of the intervertebral disc space. The disc material may be nucleus, cartilage, fragmented apophyseal bone, annular tissue, or any combination thereof. The disc space is defined craniad and caudad by the vertebral body end plates and, peripherally, by the outer edges of the vertebral ring apophyses, exclusive of osteophytes. The term ‘‘localized’’ or ‘‘focal’’ refers to the extension of the disc material less than 25% (90°) of the periphery of the disc as viewed in the axial plane.
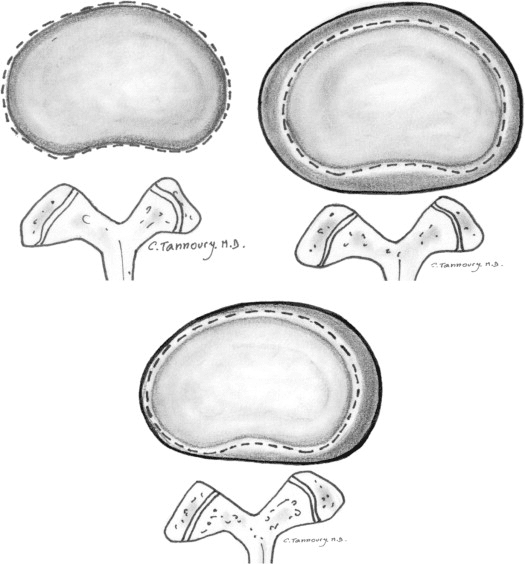
The presence of disc tissue extending beyond the edges of the ring apophyses, throughout the circumference of the disc, is called ‘‘bulging’’ and is not considered a form of herniation (Fig. 3, Top Right). Asymmetric bulging of disc tissue greater than 25% of the disc circumference (Fig. 3, Bottom), often seen as an adaptation to adjacent deformity, is, also, not a form of herniation. In evaluating the shape of the disc for a herniation in an axial plane, the shape of the two adjacent vertebrae must be considered [15, 35].
Herniated discs may be classified as protrusion or extrusion, based on the shape of the displaced material.
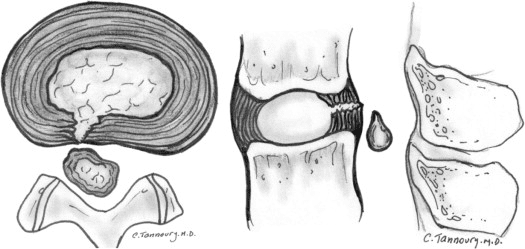
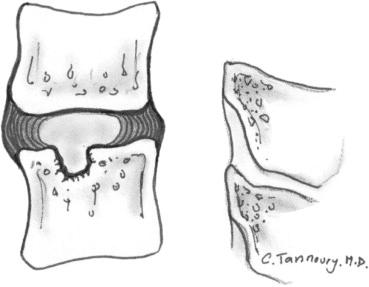
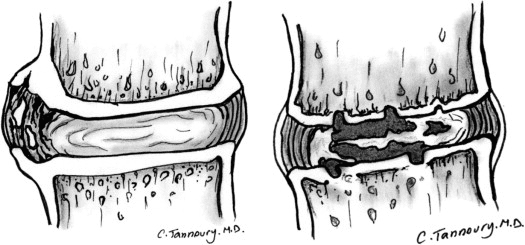
Protrusion is present if the greatest distance between the edges of the disc material presenting outside the disc space is less than the distance between the edges of the base of that disc material extending outside the disc space. The base is defined as the width of disc material at the outer margin of the disc space of origin, where disc material displaced beyond the disc space is continuous with the disc material within the disc space (Fig. 4). Extrusion is present when, in at least one plane, any one distance between the edges of the disc material beyond the disc space is greater than the distance between the edges of the base of the disc material beyond the disc space or when no continuity exists between the disc material beyond the disc space and that within the disc space (Fig. 5). The latter form of extrusion is best further specified or subclassified as sequestration if the displaced disc material has lost continuity completely with the parent disc (Fig. 6). The term migration may be used to signify displacement of disc material away from the site of extrusion. Herniated discs in the craniocaudad (vertical) direction through a gap in the vertebral body end plate are referred to as intravertebral herniations (Schmorl nodes) (Fig. 7).
Disc herniations may be further specifically categorized as contained, if the displaced portion is covered by outer annulus fibers and/or the posterior longitudinal ligament, or uncontained when absent of any such covering. If the margins of the disc protrusion are smooth on axial computed tomography (CT) or magnetic resonance imaging (MRI), then the displaced disc material is likely contained by the posterior longitudinal ligament and perhaps a few superficial posterior annular fibers [21, 35, 36, 37]. If the posterior margin of the disc protrusion is irregular, the herniation is likely uncontained. Displaced disc tissue is typically described by location, volume, and content, as discussed later in this document.
An alternative scheme of distinguishing protrusion from extrusion is discussed in the Discussion section.
Trauma
The category of trauma includes disruption of the disc associated with physical and/or imaging evidence of violent fracture and/or dislocation and does not include repetitive injury, contribution of less than violent trauma to the degenerative process, fragmentation of the ring apophysis in conjunction with disc herniation, or disc abnormalities in association with degenerative subluxations. Whether or not a ‘‘less than violent’’ injury has contributed to or been superimposed on a degenerative change is a clinical judgment that cannot be made based on images alone; therefore, from the standpoint of description of images, such discs, in the absence of significant imaging evidence of associated violent injury, should be classified as degeneration rather than trauma.
Inflammation/Infection
The category of inflammation/infection includes infection, infection-like inflammatory discitis, and inflammatory response to spondyloarthropathy. It also includes inflammatory spondylitis of the subchondral end plate and bone marrow manifested by Modic Type I MRI changes [29, 30, 38] and usually associated with degenerative pathologic changes in the disc. To simplify the classification scheme, the category is inclusive of disparate conditions; therefore, when data permit, the diagnosis should be subcategorized for appropriate specificity.
Neoplasia
Primary or metastatic morphologic changes of disc tissues caused by malignancy are categorized as neoplasia, with subcategorization for appropriate specificity.
Miscellaneous Paradiscal Masses of Uncertain Origin
Although most intraspinal cysts are of meningeal or synovial origin, a minority arise from the disc and create a
Morphologic Variant of Unknown Significance
Instances in which data suggest abnormal morphology of the disc, but in which data are not complete enough to support a diagnostic categorization can be categorized as a morphologic variant of unknown significance.
Discussion of Nomenclature in Detail
This document provides a nomenclature that facilitates the description of surgical, endoscopic, or cadaveric findings as well as imaging findings; and also, with the caveat that it addresses only the morphology of the disc, it facilitates communication for patients, families, employers, insurers, and legal and social authorities and permits accumulation of more reliable data for research.
Normal Disc
Categorization of a disc as ‘‘normal’’ means the disc is fully and normally developed and free of any changes of disease, trauma, or aging. Only the morphology, and not the clinical context, is considered. Clinically ‘‘normal’’ (asymptomatic) people may have a variety of harmless imaging findings, including congenital or developmental variations of discs, minor bulging of the annuli, age-related desiccation, anterior and lateral marginal vertebral body osteophytes, prominence of disc material beyond one end plate as a result of luxation of one vertebral body relative to the adjacent vertebral body (especially common at L5–S1), and so on [39]. By this article’s morphology-based nomenclature and classification, however, such individual discs are not considered ‘‘normal,’’ but rather are described by their morphologic characteristics, independent of their clinical import unless otherwise specified.
Disc with Fissures of the Annulus
There is a general agreement about the various forms of loss of integrity of the annulus, such as radial, transverse, and concentric fissures. Yu et al. [40] have shown that annular fissures, including radial, concentric, and transverse types, are present in nearly all degenerated discs [41]. If the disc is dehydrated on an MRI scan, it is likely that there is at least one or more small fissures in the annulus. Relatively wide, radially directed annular fissures, with stretch of the residual annular margin, at times involving avulsion of an annular fragment, have sometimes been called ‘‘annular gaps,’’ although the term is relatively new and not accepted as a standard [27].
The terms ‘‘annular fissure’’ and ‘‘annular tear’’ have been applied to the findings on T2-weighted MRI scans of localized high intensity zones (HIZ) within the annulus [30, 42, 43, 44]. High intensity zones represent fluid and/or granulation tissue and may enhance with gadolinium. Fissures occur in all degenerative discs but are not all visualized as HIZs. Discography reveals some fissures not seen by the MRI, but not all fissures are visualized by discography. Description of the imaging findings is most accurate when limited to the observation of an HIZ or discographically demonstrated fissure, with the understood caveat that there is an incomplete concordance with the HIZs, discogram images, and anatomically observed fissures.
As far back as the 1995 NASS document, authors have recommended that such lesions be termed ‘‘fissures’’ rather than ‘‘tears,’’ primarily out of concern that the word ‘‘tear’’ could be misconstrued as implying a traumatic etiology [9, 30, 45, 46]. Because of potential misunderstanding of the term ‘‘annular tear,’’ and consequent presumption that the finding of an annular fissure indicates that there has been an injury, the term ‘‘annular tear’’ should be considered nonstandard and ‘‘annular fissure’’ be the preferred term. Imaging observation of an annular fissure does not imply an injury or related symptoms, but simply defines the morphologic change in the annulus.
Degenerated Disc
Because there is a confusion in the differentiation of changes of pathologic degenerative processes in the disc from those of normal aging [17, 31, 47, 48, 49], the classification ‘‘degenerated disc’’ includes all such changes, thus does not compel the observer to differentiate the pathologic from the normal consequence of aging.
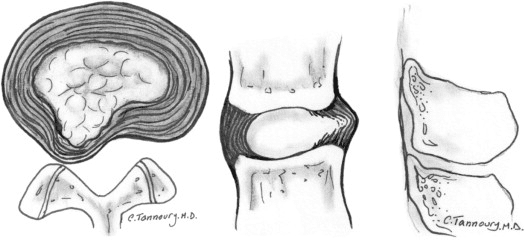
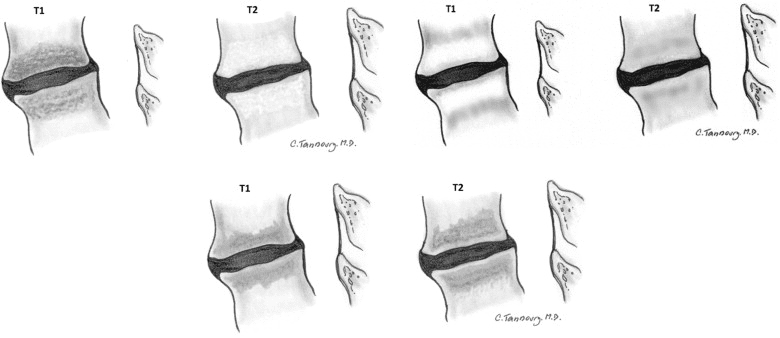
Perceptions of what constitutes the normal aging process of the spine have been greatly influenced by postmortem anatomic studies involving a limited number of specimens, harvested from cadavers from different age groups, with unknown past medical histories and the presumption of absence of lumbar symptoms [23, 50, 51, 52, 53, 54, 55, 56, 57]. With such methods, pathologic change is easily confused with consequences of normal aging. Resnick and Niwayama [31] emphasized the differentiating features of two degenerative processes involving the intervertebral disc that had been previously described by Schmorl and Junghanns [58]; ‘‘spondylosis deformans,’’ which affects essentially the annulus fibrosus and adjacent apophyses (Fig. 8, Left) and ‘‘intervertebral osteochondrosis,’’ which affects mainly the nucleus pulposus and the vertebral body end plates and may include extensive fissuring of the annulus fibrosus that may be followed by atrophy (Fig. 8, Right). Although Resnick and Niwayama stated that the cause of the two entities was unknown, other studies suggest that spondylosis deformans is the consequence of normal aging, whereas intervertebral osteochondrosis, sometimes also called ‘‘deteriorated disc,’’ results from a clearly pathologic, although not necessarily symptomatic, process [29, 31, 42, 59, 60].
Degrees of disc degeneration have been graded based on gross morphology of midsagittal sections of the lumbar spine (Thompson scheme) [19]; postdiscography CT observations of integrity of the interior of the disc (Dallas classification) (Fig. 9) [42]; MRI observations of vertebral body marrow changes adjacent to the disc (Modic classification) [30], (Fig. 10); and MRI-revealed changes in the nucleus (Pfirrmann classification) [61]. Various modifications of these schemes have been proposed to suit specific clinical and research needs [17, 35, 62, 63].
Herniated Disc
The needs of common practices make necessary a diagnostic term that describes disc material beyond the intervertebral disc space. Herniated disc, herniated nucleus pulposus (HNP), ruptured disc, prolapsed disc (used nonspecifically), protruded disc (used nonspecifically), and bulging disc (used nonspecifically) have all been used in the literature in various ways to denote imprecisely defined displacement of disc material beyond the interspace. The absence of clear understanding of the meaning of these terms and the lack of definition of limits that should be placed on an ideal general term have created a great deal of confusion in clinical practice and in attempts to make meaningful comparisons of research studies.
For the general diagnosis of displacement of disc material, the single term that is most commonly used and creates least confusion is ‘‘herniated disc.’’ ‘‘Herniated nucleus pulposus’’ is inaccurate because materials other than nucleus (cartilage, fragmented apophyseal bone, and fragmented annulus) are common components of displaced disc material [64]. ‘‘Rupture’’ casts an image of tearing apart and therefore carries more implication of traumatic etiology than ‘‘herniation,’’ which conveys an image of displacement rather than disruption.
Though ‘‘protrusion’’ has been used by some authors in a nonspecific general sense to signify any displacement, the term has a more commonly used specific meaning for which it is best reserved. ‘‘Prolapse,’’ which has been used as a general term, as synonymous with the specific meaning of protrusion, or to denote inferior migration of extruded disc material, is not frequently used in a way to provide specific meaning and is best regarded as nonstandard, in deference to the more specific terms ‘‘protrusion’’ and ‘‘extrusion.’’
By exclusion of other terms, and by reasons of simplicity and common usage, ‘‘herniated disc’’ is the best general term to denote displacement of disc material. The term is appropriate to denote the general diagnostic category when referring to a specific disc and to be inclusive of various types of displacements when speaking of groups of discs. The term includes discs that may properly be characterized by more specific terms, such as ‘‘protruded disc’’ or ‘‘extruded disc.’’ The term ‘‘herniated disc,’’ as defined in this work, refers to localized displacement of nucleus, cartilage, fragmented apophyseal bone, or fragmented annular tissue beyond the intervertebral disc space. ‘‘Localized’’ is defined as less than 25% of the disc circumference. The disc space is defined, craniad and caudad, by the vertebral body end plates and, peripherally, by the edges of the vertebral ring apophyses, exclusive of the osteophyte formation. This definition was deemed more practical, especially for the interpretation of imaging studies, than a pathologic definition requiring identification of disc material forced out of normal position through an annular defect. Displacement of disc material, either through a fracture or defect in the bony end plate or in conjunction with displaced fragments of fractured walls of the vertebral body, may be described as ‘‘herniated’’ disc, although such description should accompany description of the fracture so as to avoid confusion with primary herniation of disc material. Displacement of disc materials from one location to another within the interspace, as with intraannular migration of nucleus without displacement beyond the interspace, is not considered herniation.
To be considered ‘‘herniated,’’ disc material must be displaced from its normal location and not simply represent an acquired growth beyond the edges of the apophyses, as is the case when connective tissues develop in gaps between osteophytes or when annular tissue is displaced behind one vertebra as an adaptation to subluxation. Herniation, therefore, can only occur in association with disruption of the normal annulus or, as in the case of intravertebral herniation (Schmorl node), a defect in the vertebral body end plate.
Details of the internal architecture of the annulus are most often not visualized by even the best quality MRIs [21]. The distinction of herniation is made by the observation of displacement of disc material beyond the edges of the ring apophysis that is ‘‘focal’’ or ‘‘localized,’’ meaning less than 25% of the circumference of the disc. The 25% cutoff line is established by way of convention to lend precision to terminology and does not designate etiology, relation to symptoms, or treatment indications.
The terms ‘‘bulge’’ or ‘‘bulging’’ refer to a generalized extension of disc tissue beyond the edges of the apophyses [65]. Such bulging involves greater than 25% of the circumference of the disc and typically extends a relatively short distance, usually less than 3 mm, beyond the edges of the apophyses (Fig. 3). ‘‘Bulge’’ or ‘‘bulging’’ describes a morphologic characteristic of various possible causes. Bulging is sometimes a normal variant (usually at L5–S1), can result from an advanced disc degeneration or from a vertebral body remodeling (as consequent to osteoporosis, trauma, or adjacent structure deformity), can occur with ligamentous laxity in response to loading or angular motion, can be an illusion caused by posterior central subligamentous disc protrusion, or can be an illusion from volume averaging (particularly with CT axial images).
Bulging, by definition, is not a herniation. Application of the term ‘‘bulging’’ to a disc does not imply any knowledge of etiology, prognosis, or need for treatment or imply the presence of symptoms.
A disc may have, simultaneously, more than one herniation. A disc herniation may be present along with other degenerative changes, fractures, or abnormalities of the disc. The term ‘‘herniated disc’’ does not imply any knowledge of etiology, relation to symptoms, prognosis, or need for treatment.
When data are sufficient to make the distinction, a herniated disc may be more specifically characterized as ‘‘protruded’’ or ‘‘extruded.’’ These distinctions are based on the shape of the displaced material. They do not imply knowledge of the mechanism by which the changes occurred.
Protruded Discs
Disc protrusions are focal or localized abnormalities of the disc margin that involve less than 25% of the disc circumference. A disc is ‘‘protruded’’ if the greatest dimension between the edges of the disc material presenting beyond the disc space is less than the distance between the edges of the base of that disc material that extends outside the disc space. The base is defined as the width of the disc material at the outer margin of the disc space of origin, where disc material displaced beyond the disc space is continuous with the disc material within the disc space (Fig. 4). The term ‘‘protrusion’’ is only appropriate in describing herniated disc material, as discussed previously.
Extruded Discs
The term ‘‘extruded’’ is consistent with the lay language meaning of material forced from one domain to another through an aperture [37, 64]. With reference to a disc, the test of extrusion is the judgment that, in at least one plane, any one distance between the edges of the disc material beyond the disc space is greater than the distance between the edges of the base measured in the same plane or when no continuity exists between the disc material beyond the disc space and that within the disc space (Fig. 5). Extruded disc material that has no continuity with the disc of origin may be characterized as ‘‘sequestrated’’ [53, 66] (Fig. 6). A sequestrated disc is a subtype of ‘‘extruded disc’’ but, by definition, can never be a ‘‘protruded disc.’’ Extruded disc material that is displaced away from the site of extrusion, regardless of continuity with the disc, may be called ‘‘migrated,’’ a term that is useful for the interpretation of imaging studies because it is often impossible from images to know if continuity exists.
The aforementioned distinctions between protrusion and extrusion and between contained and uncontained are based on common practice and wide acceptance of the definitions in the original version of this document. Another set of criteria, espoused by some respected practitioners, defines extrusion as uncontained and protrusion as a persistence of containment, regardless of the relative dimensions of the base to displaced portion of disc material. Per these criteria, a disc extrusion can be identified by the presence of a continuous line of low signal intensity surrounding the disc herniation. They state that current advanced imaging permits this basis of distinction and that the presence or absence of containment has more clinical relevance than the morphology of the displaced material [35].
Whether their method will prove superior to the currently recommended method will be determined by future study. The use of the distinction between ‘‘protrusion’’ and ‘‘extrusion’’ is optional and some observers may prefer to use, in all cases, the more general term ‘‘herniation.’’ Further distinctions can often be made regarding containment, continuity, volume, composition, and location of the displaced disc material.
Containment, Continuity, and Migration
Herniated disc material can be ‘‘contained’’ or ‘‘uncontained.’’ The test of containment is whether the displaced disc tissues are wholly held within
Displaced disc fragments are sometimes characterized as ‘‘free.’’ A ‘‘free fragment’’ is synonymous with a ‘‘sequestrated fragment,’’ but not synonymous with ‘‘uncontained.’’ A disc fragment should be considered ‘‘free’’ or ‘‘sequestrated’’ only if there is no remaining continuity of the disc material between it and the disc of origin. A disc can be ‘‘uncontained,’’ with the loss of integrity of the posterior longitudinal ligament and the outer annulus, but still have continuity between the herniated/displaced disc material and the disc of origin.
The term ‘‘migrated’’ disc or fragment refers to the displacement of most of the displaced disc material away from the opening in the annulus through which the material has extruded. Some migrated fragments will be sequestrated, but the term ‘‘migrated’’ refers only to position and not to continuity.
The terms ‘‘capsule’’ and ‘‘subcapsular’’ have been used to refer to containment by an unspecified combination of annulus and ligament. These terms are nonpreferred.
Referring specifically to the posterior longitudinal ligament, some authors have distinguished displaced disc material as ‘‘subligamentous,’’ ‘‘extraligamentous,’’ ‘‘transligamentous,’’ or ‘‘perforated.’’ The term ‘‘subligamentous’’ is favored as an equivalent to ‘‘contained.’’
Volume and Composition of Displaced Material
A scheme to define the degree of canal compromise produced by disc displacement should be practical, objective, reasonably precise, and clinically relevant. A simple scheme that fulfills the criteria uses two-dimensional measurements taken from an axial section at the site of the most severe compromise. Canal compromise of less than one third of the canal at that section is ‘‘mild,’’ between one and two-thirds is ‘‘moderate,’’ and greater than two-thirds is ‘‘severe.’’ The same grading can be applied for foraminal involvement.
Such characterizations of volume describe only the cross-sectional area at one section and do not account for the total volume of displaced material; proximity to, compression, and distortion of neural structures; or other potentially significant features, which the observer may further detail by narrative description.
Composition of the displaced material may be characterized by terms such as nuclear, cartilaginous, bony, calcified, ossified, collagenous, scarred, desiccated, gaseous, or liquefied.
Clinical significance related to the observation of volume and composition depends on the correlation with clinical data and cannot be inferred from morphologic data alone.
Location
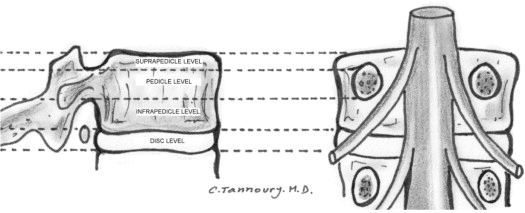
Bonneville proposed a useful and simple alphanumeric system to classify, according to location, the position of disc fragments that have migrated in the horizontal or sagittal plane [6, 13]. Using anatomic boundaries familiar to surgeons, Wiltse proposed another system [14, 67]. Anatomic ‘‘zones’’ and ‘‘levels’’ are defined using the following landmarks: medial edge of the articular facets; medial, lateral, upper, and lower borders of the pedicles; and coronal and sagittal planes at the center of the disc. On the horizontal (axial) plane, these landmarks determine the boundaries of the central zone, the subarticular zone (lateral recess), the foraminal zone, the extraforaminal zone, and the anterior zone, respectively (Fig. 11). On the sagittal (craniocaudal) plane, they determine the boundaries of the disc level, the
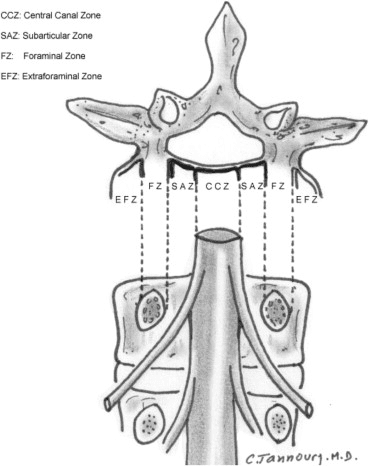
Moving from the central to right lateral in the axial (horizontal) plane, location may be defined as central, right central, right subarticular, right foraminal, or right extraforaminal. The term ‘‘paracentral’’ is less precise than defining ‘‘right central’’ or ‘‘left central,’’ but is useful in describing groups of discs that include both, or when speaking informally, when the side is not significant. For reporting of image observations of a specific disc, ‘‘right central’’ or ‘‘left central’’ should supersede the use of the term ‘‘paracentral.’’ The term ‘‘far lateral’’ is sometimes used synonymously with ‘‘extraforaminal.’’
In the sagittal plane, location may be defined as discal, infrapedicular, suprapedicular, or pedicular. In the coronal plane, anterior, in relationship to the disc, means ventral to the midcoronal plane of the centrum.
Glossary
Note: some terms and definitions included in this Glossary are not recommended as preferred terminology but are included to facilitate the interpretation of vernacular and, in some cases, improper use. Preferred definitions are listed first. Nonstandard definitions are placed in brackets, and by consensus of the organizational task forces, should not be used in the manner described. Some terms are also labeled as colloquial, with further designation as to whether they are considered nonpreferred or nonstandard.
Acute disc herniation: disc herniation of a relatively recent occurrence. Note: paradiscal inflammatory reaction and relatively bright signal of the disc material on T2-weighted images suggest relative acuteness. Such changes may persist for months, however. Thus, absent clinical correlation and/or serial studies, it is not possible to date precisely by imaging when a herniation occurred. An acutely herniated disc material may have brighter signal on T2-weighted MRI sequences than the disc from which the disc material originates [46, 59, 64, 68]. Note that a relatively acute herniation can be superimposed on a previously existing herniation. An acute disc herniation may regress spontaneously without specific treatment. See: chronic disc herniation.
Aging disc: disc demonstrating any of the various effects of aging on the disc. Loss of water content from the nucleus occurs before MRI changes, followed by the progression of MRI manifested changes consistent with the progressive loss of water content and increase in collagen and aggregating proteoglycans. See Pfirrmann classification.
Annular fissure: separations between annular fibers, separations of fibers from their vertebral body insertions, or separations of fibers that extend radially, transversely, or concentrically, involving one or many layers of the annular lamellae. Note that the terms ‘‘fissure’’ and ‘‘tear’’ have often been used synonymously in the past. The term ‘‘tear’’ is inappropriate for use in describing imaging findings and should not be used (tear: nonstandard). Neither term suggests injury or implies any knowledge of etiology, neither term implies any relationship to symptoms or that the disc is a likely pain generator, and neither term implies any need for treatment. See also: annular gap, annular rupture, annular tear, concentric fissure, HIZ, radial fissure, transverse fissure.
Annular gap (nonstandard): focal attenuation (CT) or signal (MRI) abnormality, often triangular in shape, in the posterior aspect of the disc, likely representing widening of a radially directed annular fissure, bilateral annular fissures with an avulsion of the intermediate annular fragment, or an avulsion of a focal zone of macerated annulus.
Annular rupture: disruption of fibers of the annulus by sudden violent injury. This is a clinical diagnosis; use of the term is inappropriate for a pure imaging description, which instead should focus on a detailed description of the findings. Ruptured annulus is not synonymous with ‘‘annular fissure,’’ or ‘‘ruptured disc.’’
Annular tear, torn annulus (nonstandard): see fissure of the annulus and rupture of annulus.
Anterior displacement: displacement of disc tissues beyond the disc space into the anterior zone.
Anterior zone: peridiscal zone that is anterior to the midcoronal plane of the vertebral body.
Anulus, annulus (abbreviated form of annulus fibrosus): multilaminated fibrous tissue forming the periphery of each disc space, attaching, craniad and caudad, to end plate cartilage and a ring apophyseal bone and blending centrally with the nucleus pulposus. Note: either anulus or annulus is correct spelling. Nomina Anatomica uses both forms, whereas Terminologia Anatomica states ‘‘ anulus fibrosus’’ [22]. Fibrosus has no correct alternative spelling; fibrosis has a different meaning and is incorrect in this context.
Asymmetric bulge: presence of more than 25% of the outer annulus beyond the perimeter of the adjacent vertebrae, more evident in one section of the periphery of the disc than another, but not sufficiently focal to be characterized as a protrusion. Note: asymmetric disc bulging is a morphologic observation that may have various causes and does not imply etiology or association with symptoms. See bulge.
Balloon disc (colloquial, nonstandard): diffuse apparent enlargement of the disc in superior-inferior extent because of bowing of the vertebral end plates due to weakening of the bone as in severe osteoporosis.
Base (of displaced disc): the cross-sectional area of the disc material at the outer margin of the disc space of origin, where disc material beyond the disc space is continuous with disc material within the disc space. In the craniocaudal direction, the length of the base cannot exceed, by definition, the height of the intervertebral space. On axial imaging, base refers to the width at the outer margin of the disc space, of the origin of any disc material extending beyond the disc space.
Black disc (colloquial, nonstandard): see dark disc.
Bulging disc, bulge (noun [n]), bulge (verb [v])
- A disc in which the contour of the outer annulus extends, or appears to extend, in the horizontal (axial) plane beyond the edges of the disc space, usually greater than 25% (90°) of the circumference of the disc and usually less than 3 mm beyond the edges of the vertebral body apophysis.
- (Nonstandard) A disc in which the outer margin extends over a broad base beyond the edges of the disc space.
- (Nonstandard) Mild, diffuse, smooth displacement of
disc . - (Nonstandard) Any disc displacement at the discal level.
Note: bulging is an observation of the contour of the outer disc and is not a specific diagnosis. Bulging has been variously ascribed to redundancy of the annulus, secondary to the loss of disc space height, ligamentous laxity, response to loading or angular motion, remodeling in response to adjacent pathology, unrecognized and atypical herniation, and illusion from volume averaging on CT axial images. Mild symmetric posterior disc bulging may be a normal finding at L5–S1. Bulging may or may not represent pathologic change, physiologic variant, or normalcy. Bulging is not a form of herniation; discs known to be herniated should be diagnosed as herniation or, when appropriate, as specific types of herniation. See: herniated disc, protruded disc, extruded disc.
Calcified disc: calcification within the disc space, not inclusive of osteophytes at the periphery of the disc space.
Cavitation: spaces, cysts, clefts, or cavities formed within the nucleus and inner annulus from disc degeneration.
See vacuum disc.
Central zone: zone within the vertebral canal between sagittal planes through the medial edges of each facet. Note: the center of the central zone is a sagittal plane through the center of the vertebral body. The zones to either side of the center plane are right central and left central, which are preferred terms when the side is known, as when reporting imaging results of a specific disc. When the side is unspecified, or grouped with both right and left represented, the term paracentral is appropriate.
Chronic disc herniation: a clinical distinction that a disc herniation is of long duration. There are no universally accepted definitions of the intervals that distinguish between acute, subacute, and chronic disc herniations. Serial MRIs revealing disc herniations that are unchanged in appearance over time may be characterized as chronic. Disc herniations associated with calcification or gas on CT may be suggested as being chronic. Even so, the presence of calcification or gas does not rule out an acutely herniated disc. Note that an acute disc herniation may be superimposed on a chronic disc herniation. Magnetic resonance imaging signal characteristics may, on rare occasion, allow differentiation of acute and chronic disc herniations [16, 59, 64]. In such cases, acutely herniated disc material may appear brighter than the disc of origin on T2-weighted sequences [46, 59, 61]. Also, see disc-osteophyte complex.
Claw osteophyte: bony outgrowth arising very close to the disc margin, from the vertebral body apophysis, directed, with a sweeping configuration, toward the corresponding part of the vertebral body opposite the disc.
Collagenized disc or nucleus: a disc in which the mucopolysaccharide of the nucleus has been replaced by fibrous tissue.
Communicating disc, communication (n), communicate (v) (nonstandard): communication refers to interruption in the periphery of the disc annulus, permitting free passage of fluid injected within the disc to the exterior of the disc, as may be observed during discography. Not synonymous with ‘‘uncontained.’’ See ‘‘contained disc’’ and ‘‘uncontained disc.’’
Concentric fissure: fissure of the annulus characterized by separation of annular fibers in a plane roughly parallel to the curve of the periphery of the disc, creating fluid-filled spaces between adjacent annular lamellae. See: radial fissures, transverse fissures, HIZ.
Contained herniation, containment (n), contain (v)
- Displaced disc tissue existing wholly within an outer perimeter of
uninterrupted outer annulus or posterior longitudinal ligament. - (Nonstandard) A disc with its contents mostly, but not wholly, within annulus or capsule.
- (Nonstandard) A disc with displaced elements contained within any investiture of the vertebral canal.
A disc that is less than wholly contained by annulus, but under a distinct posterior longitudinal ligament, is contained. Designation as ‘‘contained’’ or ‘‘uncontained’’ defines the integrity of the ligamentous structures surrounding the disc, a distinction that is often but not always possible by advanced imaging. On CT and MRI scans, contained herniations typically have a smooth margin, whereas uncontained herniations most often have irregular margins because the outer annulus and the posterior longitudinal ligament have been penetrated by the disc material [35, 37]. CT-discography also does not always allow one to distinguish whether the herniated components of a disc are contained, but only whether there is communication between the disc space and the vertebral canal.
Continuity: connection of displaced disc tissue by a bridge of disc tissue, however thin, to tissue within the disc of origin.
Dallas classification (of postdiscography imaging): commonly used grading system for the degree of annular fissuring seen on CT imaging of discs after discography. Dallas Grade 0 is normal; Grade 1: leakage of contrast into the inner one-third of the annulus; Grade 2: leakage of contrast into the inner two-thirds of the annulus; Grade 3: leakage through the entire thickness of the annulus; Grade 4: contrast extends circumferentially; Grade 5: contrast extravasates into the epidural space (See discogram, discography).
Dark disc (colloquial, nonstandard): disc with nucleus showing decreased signal intensity on T2-weighted images (dark), usually because of desiccation of the nucleus secondary to degeneration. Also: black disc (colloquial, nonstandard). See: disc degeneration, Pfirrmann classification.
Degenerated disc, degeneration (n), degenerate (v)
- Changes in a disc characterized to varying degrees by one or more of the following: desiccation, cleft formation, fibrosis, and gaseous degradation of the nucleus; mucinous degradation, fissuring, and loss of integrity of the annulus; defects in and/or sclerosis of the end plates; and osteophytes at the vertebral apophyses.
- Imaging manifestation of such changes, including [35] standard roentgenographic findings, such as disc space narrowing and
peridiscal osteophytes, MRI disc findings (see Pfirrmann classification [61]), CT disc findings (see discogram/discography and Dallas classification [42]), and/or MRI findings of vertebralend plate and marrow reactive changes adjacent to a disc (see Modic classification [38]).
Degenerative disc disease (nonstandard term when used as an imaging description): a condition characterized by manifestations of disc degeneration and symptoms thought to be related to those of degenerative changes. Note: causal connections between degenerative changes and symptoms are often difficult clinical distinctions. The term ‘‘degenerative disc disease’’ carries implications of illness that may not be appropriate if the only or primary indicators of illness are from imaging studies, and thus this term should not be used when describing imaging findings. The preferred term for description of imaging manifestations is ‘‘degenerated disc’’ or ‘‘disc degeneration,’’ rather than ‘‘degenerative disc disease.’’
Delamination: separation of circumferential annular fibers along the planes parallel to the periphery of the disc, characterizing a concentric fissure of the annulus.
Desiccated disc
- Disc with reduced water content, usually primarily of nuclear tissues.
- Imaging manifestations of
reduced water content of the disc, such as decreased (dark) signal intensity on T2-weighted images, or ofapparent reduced water content, as from alterations in the concentration of hydrophilic glycosaminoglycans. See also: dark disc (colloquial, nonstandard).
Disc (disk): complex structure composed of nucleus pulposus, annulus fibrosus, cartilaginous end plates, and vertebral body ring apophyseal attachments of annulus. Note: most English language publications use the spelling ‘‘disc’’ more often than ‘‘disk’’ [1, 20, 22, 69, 70]. Nomina Anatomica designates the structures as ‘‘disci intervertebrales’’ and Terminologia Anatomica as ‘‘discus intervertebralis/intervertebral disc’’ [22, 70]. (See ‘‘disc level’’ for naming and numbering of a particular disc).
Disc height: The distance between the planes of the end plates of the vertebral bodies craniad and caudad to the disc. Disc height should be measured at the center of the disc, not at the periphery. If measured at the posterior or anterior margin of the disc on a sagittal image of the spine, this should be clearly specified as such.
Disc level: Level of the disc and vertebral canal between axial planes through the bony end plates of the vertebrae craniad and caudad to the disc being described.
- A particular disc is best named by naming the region of the spine and the vertebra above and below it; for example, the disc between the fourth and fifth lumbar vertebral bodies is named ‘‘lumbar 4–5,’’ commonly abbreviated as L4–L5, and the disc between the fifth lumbar vertebral body and the first sacral vertebral body is called ‘‘lumbosacral disc’’ or ‘‘L5–S1.’’ Common anomalies include patients with six lumbar vertebrae or transitional vertebrae at the lumbosacral junction that require, for clarity,
narrative explanation of the naming of the discs. - (Nonstandard) A disc is sometimes labeled by the vertebral body above it; for example, the disc between L4 and L5 may be labeled ‘‘the L4 disc’’.
- Note: ‘‘a motion segment,’’ numbered in the same way, is a functional unit of the spine, comprising the vertebral body above and below, the disc, the facet joints, and the connecting soft tissues and is most often referenced with regard to the stability of the spine.
Disc of origin: disc from which a displaced fragment originated. Synonym: parent disc. Note: since displaced fragments often contain tissues other than nucleus, disc of origin is preferred to nucleus of origin. Parent disc is synonymous, but more colloquial and nonpreferred.
Disc space: space limited, craniad and caudad, by the end plates of the vertebrae and peripherally by the edges of the vertebral body ring apophyses, exclusive of osteophytes. Synonym: intervertebral disc space. See ‘‘disc’’ level for naming and numbering of discs.
Discogenic vertebral sclerosis: increased bone density and calcification adjacent to the end plates of the vertebrae, craniad and caudad, to a degenerated disc, sometimes associated with intervertebral osteochondrosis. Manifested on MRI as Modic Type III.
Discogram, discography: a diagnostic procedure in which contrast material is injected into the nucleus of the disc with radiographic guidance and observation, often followed by CT/discogram. The procedure is often accompanied by pressure measurements and assessment of pain response (provocative discography). The degree of annular fissuring identified by discography may be defined by the Dallas classification and its modifications (See Dallas classification).
Disc-osteophyte complex: intervertebral disc displacement, whether bulge, protrusion, or extrusion, associated with calcific ridges or ossification. Sometimes called a hard disc or chronic disc herniation (nonpreferred). Distinction should be made between ‘‘spondylotic disc herniation,’’ or ‘‘calcified disc herniation’’ (nonpreferred), the remnants of an old disc herniation; and ‘‘spondylotic bulging disc,’’ a broad-based bony ridge presumably related to chronic bulging disc.
Displaced disc (nonstandard): a disc in which disc material is beyond the outer edges of the vertebral body ring apophyses (exclusive of osteophytes) of the craniad and caudad vertebrae, or, as in the case of intravertebral herniation, has penetrated through the vertebral body end plate.
Note: displaced disc is a general term that does not imply knowledge of the underlying pathology, cause, relationship to symptoms, or need for treatment. The term includes, but is not limited to, disc herniation and disc migration. See: herniated disc, migrated disc.
Epidural membrane: See peridural membrane.
Extraforaminal zone: the peridiscal zone beyond the sagittal plane of the lateral edges of the pedicles, having no well-defined lateral border, but definitely posterior to the anterior zone. Synonym: ‘‘far lateral zone,’’ also ‘‘far-out zone’’ (nonstandard).
Extraligamentous: posterior or lateral to the posterior longitudinal ligament. Note: extraligamentous disc refers to displaced disc tissue that is located posterior or lateral to the posterior longitudinal ligament. If the disc has extruded through the posterior longitudinal ligament, it is sometimes called ‘‘transligamentous’’ or ‘‘perforated’’ and if through the peridural membrane, it is sometimes refined to ‘‘transmembranous.’’
Extruded disc, extrusion (n), extrude (v): a herniated disc in which, in at least one plane, any one distance between the edges of the disc material beyond the disc space is greater than the distance between the edges of the base of the disc material beyond the disc space in the same plane or when no continuity exists between the disc material beyond the disc space and that within the disc space. Note: the preferred definition is consistent with the common image of extrusion, as an expulsion of material from a container through and beyond an aperture. Displacement beyond the outer annulus of the disc material with any distance between its edges greater than the distance between the edges of the base distinguishes extrusion from protrusion. Distinguishing extrusion from protrusion by imaging is best done by measuring the edges of the displaced material and the remaining continuity with the disc of origin, whereas relationship of the displaced portion to the aperture through which it has passed is more readily observed surgically. Characteristics of protrusion and extrusion may coexist, in which case the disc should be subcategorized as extruded. Extruded discs in which all continuity with the disc of origin is lost may be further characterized as ‘‘sequestrated.’’ Disc material displaced away from the site of extrusion may be characterized as ‘‘migrated.’’ See: herniated disc, migrated disc, protruded disc.
Note: An alternative scheme is espoused by some respected radiologists who believe it has better clinical application. This scheme defines extruded disc as synonymous with “uncontained disc” and does not use comparative measurements of the base versus the displaced material. Per this definition, a disc extrusion can be identified by the presence of a continuous line of low signal intensity surrounding the disc herniation. Future study will further determine the validity of this alternative definition. See: contained disc.
Far lateral zone: the peridiscal zone beyond the sagittal plane of the lateral edge of the pedicle, having no well defined lateral border, but definitely posterior to the anterior zone. Synonym: ‘‘extraforaminal zone.’’
Fissure of annulus: see annular fissure.
Foraminal zone: the zone between planes passing through the medial and lateral edges of the pedicles. Note: the foraminal zone is sometimes called the ‘‘pedicle zone’’ (nonstandard), which can be confusing because pedicle zone might also refer to measurements in the sagittal plane between the upper and lower surfaces of a given pedicle that is properly called the ‘‘pedicle level.’’ The foraminal zone is also sometimes called the ‘‘lateral zone’’ (nonstandard), which can be confusing because the ‘‘lateral zone’’ can be confused with ‘‘lateral recess’’ (subarticular zone) and can also mean extraforaminal zone or an area including both the foraminal and extraforaminal zones.
Free fragment
- A fragment of disc that has separated from the disc of origin and has no continuous bridge of disc tissue with disc tissue within the disc of origin. Synonym: sequestrated disc.
- (Nonstandard) A fragment that is not contained within the outer perimeter of the annulus.
- (Nonstandard) A fragment that is not contained within the annulus, posterior longitudinal ligament, or peridural membrane.
Note: ‘‘sequestrated disc’’ and ‘‘free fragment’’ are virtually synonymous. When referring to the condition of the disc, categorization as extruded with subcategorization as sequestrated is preferred, whereas when referring specifically to the fragment, free fragment is preferred.
Gap of annulus: see annular gap.
Hard disc (colloquial): disc displacement in which the displaced portion has undergone calcification or ossification and may be intimately associated with apophyseal osteophytes. Note: the term ‘‘hard disc’’ is most often used in reference to the cervical spine to distinguish chronic hypertrophic and reactive changes at the periphery of the disc from the more acute extrusion of soft, predominantly nuclear tissue. See: chronic disc herniation, disc-osteophyte complex.
Herniated disc, herniation (n), herniated (v): localized or focal displacement of disc material beyond the normal margin of the intervertebral disc space. Note: ‘‘localized’’ or ‘‘focal’’ means, by way of convention, less than 25% (90°) of the circumference of the disc.
Herniated disc material may include nucleus pulposus, cartilage, fragmented apophyseal bone, or annulus fibrosus tissue. The normal margins of the intervertebral disc space are defined, craniad and caudad, by the vertebral body end plates and peripherally by the edges of the vertebral body ring apophyses, exclusive of osteophytic formations. Herniated disc generally refers to displacement of disc tissues through a disruption in the annulus, the exception being intravertebral herniations (Schmorl nodes) in which the displacement is through the vertebral end plate. Herniated discs may be further subcategorized as protruded or extruded. Herniated disc is sometimes referred to as HNP, but the term ‘‘herniated disc’’ is preferred because displaced disc tissues often include cartilage, bone fragments, or annular tissues. The terms ‘‘prolapse’’ and ‘‘rupture’’ when referring to disc herniations are nonstandard and their use should be discontinued. Note: ‘‘herniated disc’’ is a term that does not imply knowledge of the underlying pathology, cause, relationship to symptoms, or need for treatment.
Herniated nucleus pulposus (HNP, nonpreferred): see herniated disc.
High intensity zone (HIZ): area of high intensity on T2-weighted MRIs of the disc, located commonly in the outer annulus. Note: HIZs within the posterior annular substance may indicate the presence of an annular fissure within the annulus, but these terms are not synonymous. An HIZ itself may represent the actual annular fissure or alternatively, may represent vascularized fibrous tissue (granulation tissue) within the substance of the disc in an area adjacent to a fissure. The visualization of an HIZ does not imply a traumatic etiology or that the disc is a source of pain.
Infrapedicular level: the level between the axial planes of the inferior edges of the pedicles craniad to the disc in question and the inferior end plate of the vertebral body above the disc in question. Synonym: superior vertebral notch.
Internal disc disruption: disorganization of structures within the disc. See intraannular displacement
Interspace: see disc space.
Intervertebral chondrosis: see intervertebral osteochondrosis.
Intervertebral disc: see disc.
Intervertebral disc space: see disc space.
Intervertebral osteochondrosis: degenerative process of the disc and vertebral body end plates that is characterized by disc space narrowing, vacuum phenomenon, and vertebral body reactive changes. Synonym: osteochondrosis (nonstandard).
Intraannular displacement: displacement of central, predominantly nuclear, tissue to a more peripheral site within the disc space, usually into a fissure in the annulus. Synonym: (nonstandard) intraannular herniation, intradiscal herniation. Note: intraannular displacement is distinguished from disc herniation, that is, herniation of disc refers to displacement of disc tissues beyond the disc space. Intraannular displacement is a form of internal disruption. When referring to intraannular displacement, it is best not to use the term ‘‘herniation’’ to avoid confusion with disc herniation.
Intraannular herniation (nonstandard): see intraannular displacement.
Intradiscal herniation (nonstandard): see intraannular displacement.
Intradural herniation: disc material that has penetrated the dura so that it lies in an intradural extramedullary location.
Intravertebral herniation: a disc displacement in which a portion of the disc projects through the vertebral end plate into the centrum of the vertebral body. Synonym: Schmorl node.
Lateral recess: that portion of the subarticular zone that is medial to the medial border of the pedicle. It refers to the entire cephalad-caudad region that exists medial to the pedicle, where the same numbered thoracic or lumbar nerve root travels caudally before exiting the nerve root foramen under the caudal margin of the pedicle. It does not refer to the nerve root foramen itself. See also subarticular zone.
Lateral zone (nonstandard): see foraminal zone.
Leaking disc (nonstandard): see communicating disc.
Limbus vertebra: separation of a segment of vertebral ring apophysis. Note: limbus vertebra may be a developmental abnormality caused by failure of integration of the ossifying apophysis to the vertebral body; a chronic herniation (extrusion) of the disc into the vertebral body at the junction of the fusing apophyseal ring, with separation of a portion of the ring with bony displacement; or a fracture through the apophyseal ring associated with intrabody disc herniation. This occurs in children before the apophyseal ring fuses to the vertebral body. In adults, a limbus vertebra should not be confused with an acute fracture. A limbus vertebra does not imply that there has been an injury to the disc or the adjacent apophyseal end plate.
Marginal osteophyte: osteophyte that protrudes from and beyond the outer perimeter of the vertebral end plate apophysis.
Marrow changes (of vertebral body): see Modic classification.
Migrated disc, migration (n), migrate (v)
- 1.Herniated disc in which a portion of the extruded disc material is displaced away from the fissure in the outer annulus through which it has extruded in either sagittal or axial plane.
- 2.(Nonstandard) A herniated disc with a free fragment or sequestrum beyond the disc level.
Note: migration refers to the position of the displaced disc material, rather than to its continuity with disc tissue within the disc of origin; therefore, it is not synonymous with sequestration.
Modic classification (Type I, II, and III) [30]: a classification of degenerative changes involving the vertebral end plates and adjacent vertebral bodies associated with disc inflammation and degenerative disc disease, as seen on MRIs. Type I refers to decreased signal intensity on T1-weighted spin echo images and increased signal intensity on T2-weighted images, representing penetration of the end plate by fibrovascular tissue, inflammatory changes, and perhaps edema. Type I changes may be chronic or acute. Type II refers to increased signal intensity on T1-weighted images and isointense or increased signal intensity on T2-weighted images, indicating replacement of normal bone marrow by fat. Type III refers to decreased signal intensity on both T1-and T2-weighted images, indicating reactive osteosclerosis (See: discogenic vertebral sclerosis).
Motion segment: the functional unit of the spine. See disc level.
Nonmarginal osteophyte: an osteophyte that occurs at sites other than the vertebral end plate apophysis. See: marginal osteophyte.
Normal disc: a fully and normally developed disc with no changes attributable to trauma, disease, degeneration, or aging. Note: many congenital and developmental variations may be clinically normal; that is, they are not associated with symptoms, and certain adaptive changes in the disc may be normal considering adjacent pathology; however, classification and reporting for medical purposes is best served if such discs are not considered normal. Note, however, that a disc finding considered not normal does not necessarily imply a cause for clinical signs or symtomatology; the description of any variation of the disc is independent of clinical judgment regarding what is normal for a given patient.
Nucleus of origin (nonpreferred): the central, nuclear portion of the disc of reference, usually used to reference the disc from which the tissue has been displaced. Note: since displaced fragments often contain tissues other than the nucleus, disc of origin is preferred to nucleus of origin. Synonym: disc of origin (preferred), parent nucleus (nonpreferred).
Osteochondrosis: see intervertebral osteochondrosis.
Osteophyte: focal hypertrophy of the bone surface and/or ossification of the soft tissue attachment to the bone.
Paracentral: in the right or left central zone of the vertebral canal. See central zone. Note: the terms ‘‘right central’’ or ‘‘left central’’ are preferable when speaking of a single site when the side can be specified, as when reporting the findings of imaging procedures. ‘‘Paracentral’’ is appropriate if the side is not significant or when speaking of mixed sites.
Parent disc (nonpreferred): see disc of origin.
Parent nucleus (nonpreferred): see nucleus of origin, disc of origin.
Pedicular level: the space between the axial planes through the upper and lower edges of the pedicle. Note: the pedicular level may be further designated with reference to the disc in question as ‘‘pedicular level above’’ or ‘‘pedicular level below’’ the disc in question.
Perforated (nonstandard): see transligamentous.
Peridural membrane: a delicate, translucent membrane that attaches to the undersurface of the deep layer of the posterior longitudinal ligament, and extends laterally and posteriorly, encircling the bony spinal canal outside the dura. The veins of Batson plexus lie on the dorsal surface of the peridural membrane and pierce it ventrally. Synonym: lateral membrane, epidural membrane.
Pfirrmann classification: a grading system for the severity of degenerative changes within the nucleus of the intervertebral disc. A Pfirrmann Grade I disc has a uniform high signal in the nucleus on T2-weighted MRI; Grade II shows a central horizontal line of low signal intensity on sagittal images; Grade III shows high intensity in the central part of the nucleus with lower intensity in the peripheral regions of the nucleus; Grade IV shows low signal intensity centrally and blurring of the distinction between nucleus and annulus; and Grade V shows homogeneous low signal with no distinction between nucleus and annulus.[61]
Prolapsed disc, prolapse (n, v) (nonstandard): the term is variously used to refer to herniated discs. Its use is not standardized and the term does not add to the precision of disc description, so is regarded as nonstandard in deference to ‘‘protrusion’’ or ‘‘extrusion.’’
Protruded disc, protrusion (n), protrude (v): 1. One of the two subcategories of a ‘‘herniated disc’’ (the other being an ‘‘extruded disc’’) in which disc tissue extends beyond the margin of the disc space, involving less than 25% of the circumference of the disc margin as viewed in the axial plane. The test of protrusion is that there must be localized (less than 25% of the circumference of the disc) displacement of disc tissue and the distance between the corresponding edges of the displaced portion must not be greater than the distance between the edges of the base of the displaced disc material at the disc space of origin (See base of displaced disc). While sometimes used as a general term in the way herniation is defined, the use of the term ‘‘protrusion’’ is best reserved for subcategorization of herniation meeting the above criteria. 2. (nonstandard) Any or unspecified type of disc herniation.
Radial fissure: disruption of annular fibers extending from the nucleus outward toward the periphery of the annulus, usually in the craniad-caudad (vertical) plane, although, at times, with axial horizontal (transverse) components. ‘‘Fissure’’ is the preferred term to the nonstandard term ‘‘tear.’’ Neither term implies knowledge of injury or other etiology. Note: Occasionally, a radial fissure extends in the transverse plane to include an avulsion of the outer layers of annulus from the apophyseal ring. See concentric fissures, transverse fissures.
Rim lesion (nonstandard): See limbus vertebra.
Rupture of annulus, ruptured annulus: see annular rupture.
Ruptured disc, rupture (nonstandard): a herniated disc. The term ‘‘ruptured disc’’ is an improper synonym for herniated disc, not to be confused with violent disruption of the annulus related to injury. Its use should be discontinued.
Schmorl node: see intravertebral herniation.
Sequestrated disc, sequestration (n), sequestrate (v); (variant: sequestered disc): an extruded disc in which a portion of the disc tissue is displaced beyond the outer annulus and maintains no connection by disc tissue with the disc of origin. Note: an extruded disc may be subcategorized as ‘‘sequestrated’’ if no disc tissue bridges the displaced portion and the tissues of the disc of origin. If even a tenuous connection by disc tissue remains between a displaced fragment and disc of origin, the disc is not sequestrated. If a displaced fragment has no connection with the disc of origin, but is contained within peridural membrane or under a portion of posterior longitudinal ligament that is not intimately bound with the annulus of origin, the disc is considered sequestrated. Sequestrated and sequestered are used interchangeably. Note: ‘‘sequestrated disc’’ and ‘‘free fragment’’ are virtually synonymous. See: free fragment. When referring to the condition of the disc, categorization as extruded with subcategorization as sequestered is preferred, whereas when referring specifically to the fragment, free fragment is preferred. See sequestrum.
Sequestrum (nonpreferred): refers to disc tissue that has displaced from the disc space of origin and lacks any continuity with disc material within the disc space of origin. Synonym: free fragment (preferred). See sequestrated disc. Note: ‘‘sequestrum’’ (nonpreferred) refers to the isolated free fragment itself, whereas sequestrated disc defines the condition of the disc.
Spondylitis: inflammatory disease of the spine, other than degenerative disease. Note: spondylitis usually refers to noninfectious inflammatory spondyloarthropathies.
Spondylosis: 1. Common nonspecific term used to describe effects generally ascribed to degenerative changes in the spine, particularly those involving hypertrophic changes to the apophyseal end plates and zygapophyseal joints. 2. (nonstandard) Spondylosis deformans, for which spondylosis is a shortened form.
Spondylosis deformans: degenerative process of the spine involving the annulus fibrosus and vertebral body apophysis, characterized by anterior and lateral marginal osteophytes arising from the vertebral body apophyses, while the intervertebral disc height is normal or only slightly decreased. See degeneration, spondylosis.
Subarticular zone: the zone, within the vertebral canal, sagittally between the plane of the medial edges of the pedicles and the plane of the medial edges of the facets and coronally between the planes of the posterior surfaces of the vertebral bodies and the anterior surfaces of the superior facets. Note: the subarticular zone cannot be precisely delineated in two-dimensional depictions because the structures that define the planes of the zone are irregular. The lateral recess is that portion of the subarticular zone defined by the medial wall of the pedicle, where the same numbered nerve root traverses before turning under the inferior wall of the pedicle into the foramen.
Subligamentous: beneath the posterior longitudinal ligament. Note: although the distinction between outer annulus and posterior longitudinal ligament may not always be identifiable, subligamentous has meaning distinct from subannular when the distinction can be made. When the distinction cannot be made, subligamentous is appropriate. Subligamentous contrasts to extraligamentous, transligamentous, or perforated. See extraligamentous, transligamentous.
Submembranous: enclosed within the peridural membrane. Note: with reference to the displaced disc material, characterization of a herniation as submembranous usually infers that the displaced portion is extruded beyond annulus and posterior longitudinal ligament so that only the peridural membrane invests it.
Suprapedicular level: the level within the vertebral canal between the axial planes of the superior end plate of the vertebra caudad to the disc space in question and the superior margin of the pedicle of that vertebra. Synonym: inferior vertebral notch.
Syndesmophytes: thin and vertically oriented bony outgrowths extending from one vertebral body to the next and representing ossification within the outer portion of the annulus fibrosus.
Tear of annulus, torn annulus (nonstandard): see annular tear.
Thompson classification: a five-point grading scale of degenerative changes in the human intervertebral disc, from 0 (normal) to 5 (severe degeneration), based on gross pathologic morphology of midsagittal sections of the lumbar spine.
Traction osteophytes: bony outgrowth arising from the vertebral body apophysis, 2 to 3 mm above or below the edge of the intervertebral disc, projecting in a horizontal direction.
Transligamentous: displacement, usually extrusion, of disc material through the posterior longitudinal ligament. Synonym: (nonstandard) (perforated). See also extraligamentous, transmembranous.
Transmembranous: displacement of extruded disc material through the peridural membrane.
Transverse fissure: fissure of the annulus in the axial (horizontal) plane. When referring to a large fissure in the axial plane, the term is synonymous with a horizontally oriented radial fissure. Often ‘‘transverse fissure’’ refers to a more limited, peripheral separation of annular fibers including attachments to the apophysis. These more narrowly defined peripheral fissures may contain gas visible on radiographs or CT images and may represent early manifestations of spondylosis deformans. See annular fissure, concentric fissure, radial fissure.
Uncontained disc: displaced disc material that is not contained by the outer annulus and/or posterior longitudinal ligament. See discussion under contained disc.
Vacuum disc: a disc with imaging findings characteristic of gas (predominantly nitrogen) in the disc space, usually a manifestation of disc degeneration.
Vertebral body marrow changes: reactive vertebral body signal changes associated with disc inflammation and disc degeneration, as seen on MRIs. See Modic classification.
Vertebral notch (inferior): incisura of the upper surface of the pedicle corresponding to the lower part of the foramen (suprapedicular level).
Vertebral notch (superior): incisura of the under surface of the pedicle corresponding to the upper part of the foramen (infrapedicular level).
Supplementary Appendix
A herniated disc most commonly develops as a result of age-related wear and tear or degeneration on the spine. In children and young adults, the intervertebral discs have a much higher water content. As we age, however, the water content of the intervertebral discs decreases and these begin to shrink while the spaces between the vertebra gets narrower, ultimately turning less flexible and becoming more prone to disc herniation. Proper diagnosis and treatment
Curated by Dr. Alex Jimenez
References
- Fardon, D.F. and Milette, P.C. Nomenclature and classification of lumbar disc pathology: recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. Spine. 2001; 26: E93–E113
- Stadnik, T.W., Lee, R.R., Coen, H.L. et al. Annular tear and disk herniation: prevalence and contrast enhancement on MR images in the absence of low back pain or sciatica. Radiology. 1998; 206: 49–55
- Mink, J.H. Terminology of lumbar spine disorders, the problem… and a solution. California Managed Imaging Medical Group Publication, Burlingame, CA; 1993
- Murtagh, F.R. The importance of being Earnest-about disk nomenclature. Am J Neuroradiol. 2007;28: 1–2
- in: E.J. Nordby, M.D. Brown, E.D. Dawson, (Eds.) A glossary on spinal terminology. American Academy of Orthopaedic Surgeons, Chicago; 1985: 31–32
- Bonneville, J.F. and Dietemann, J.L. L’imagerie
dans les sciatiques . Rev Prat (Paris). 1992; 42: 554–566 - Brant-Zawadzki, M.N. and Jensen, M.C. Imaging corner: spinal nomenclature. Inter- and intra-observer variability in interpretation of lumbar disc abnormalities: a comparison of two nomenclatures. Spine. 1995; 20: 388–390
- Breton, G. Is that a bulging disc, a small herniation, or a moderate protrusion?. Can Assoc Radiol J. 1991; 42: 318
- Fardon, D.F., Herzog, R.J., and Mink, J.H. Nomenclature of lumbar disc disorders. in: S.R. Garfin, A.R. Vaccaro (Eds.) Orthopaedic knowledge update: spine. American Academy of Orthopaedic Surgeons
,Rosemont , IL; 1997: A3–A14 - Milette, P.C. The proper terminology for reporting lumbar intervertebral disc disorders. Am J Neuroradiol. 1997; 18: 1859–1866
- Fardon DF, White AH, Wiesel S. Diagnostic terms and conservative treatments favored for lumbar disorders by spine surgeons in North America. Presented at the first annual meeting, North American Spine Society, Lake George, New York, 1986.
- Arana, E., Royuela, A., Kovacs, F.M. et al. Lumbar spine: agreement in the interpretation of 1.5T MR images by using the Nordic Modic consensus group classification form. Radiology. 2010; 254: 809–817
- Bonneville, J.F. Plaidoyer pour
une classification parl’image des hernies discales lombaires: la carte-image. Rev Im Med. 1990; 2: 557–560 - Fardon, D.F., Pinkerton, S., Balderston, R. et al. Terms used for diagnosis by English speaking spine surgeons. Spine. 1993; 18: 1–4
- Farfan, H.F., Huberdeau, R.M., and Dubow, H.I. Lumbar intervertebral disc degeneration: the influence of geometrical features on the pattern of disc degeneration: a post-mortem study. J Bone Joint Surg [Am]. 1972; 54: 492–510
- Milette, P.C., Fontaine, S., Lepanto, L. et al. Differentiating lumbar disc protrusions, disc bulges, and discs with normal contour but abnormal signal intensity. Spine. 1999; 24: 44–53
- Milette, P.C., Melancon, D., Dupuis, P. et al. A simplified terminology for abnormalities of the lumbar disc. Can Assoc Radiol J. 1991; 42: 319–325
- Taveras, J.M. Herniated intervertebral disk. A plea for a more uniform terminology. Am J Neuroradiol. 1989; 10: 1283–1284
- Thompson, J.P., Pearce, R.H., Schechter, M.T. et al. Preliminary evaluation of a scheme for grading the gross morphology of the human intervertebral disc. Spine. 1990; 15: 411–415
- Fardon, D.F., Balderston, R.A., Garfin, S.R. et al. Disorders of the spine, a coding system for diagnoses. Hanley and Belfus, Philadelphia; 1991: 20–22
- Herzog, R.J. The radiologic assessment for a lumbar disc herniation. Spine. 1996; 21: 19S–38S
- International anatomical nomenclature committee approved by Eleventh International Congress of anatomists. Nomina anatomica. 5th ed. Waverly Press, Baltimore, MD; 1983: A23
- Jarvik, J.G., Haynor, D.R., Koepsell, T.D. et al. Interreader reliability for a new classification of lumbar disc abnormalities. Acad Radiol. 1996; 3: 537–544
- Ketler, A. and Wilke, H.J. Review of existing grading systems for cervical or lumbar disc and facet joint degeneration. (with Erratum note in Eur Spine J 15(6); 729)Eur Spine J. 2006; 15: 705–718
- Kieffer, S.A., Stadlan, E.M., Mohandas, A., and Peterson, H.O. Discographic-anatomical correlation of developmental changes with age in the intervertebral disc. Acta Radiol [Diagn] (Stockholm). 1969; 9: 733–739
- Bundschuh, C.V. Imaging of the postoperative lumbosacral spine. Neuroimaging Clin N Am. 1993; 3: 499–516
- Bartynski, W.S., Rothfus, W.E., and Kurs-Lasky, M. Post-diskogram CT features of lidocaine-sensitive and lidocaine-insensitive severely painful disks at provocation lumbar diskography. AJNR. 2008; 29: 1455–1460
- Ford, L.T., Gilula, L.A., Murphy, W.A., and Gado, M. Analysis of gas in vacuum lumbar disc. AJR. 1977; 128: 1056–1057
- Modic, M.T. and Herfkens, R.J. Intervertebral disc: normal age-related changes in MR signal intensity. Radiology. 1990; 177: 332–334
- Modic, M.T., Masaryk, T.J., Ross, J.S., and Carter, J.R. Imaging of degenerative disc disease.Radiology. 1988; 168: 177–186
- Resnick, D. and Niwayama, G. Degenerative disease of the spine. in: D. Resnick (Ed.) Diagnosis of bone and joint disorders. 3rd ed. WB Saunders, Philadelphia; 1995: 1372–1462
- Eckert, C. and Decker, A. Pathological studies of intervertebral discs. J Bone Joint Surg. 1947; 29: 447–454
- Marinelli, N.L., Haughton, V.M., and Anderson, P.A. T2 relaxation times correlated with stage of lumbar disc degeneration and patient age. AJNR. 2010; 31: 1278–1282
- Yasuma, T., Koh, S., Okamura, T. et al. Histologic changes in aging lumbar intervertebral discs. J Bone Joint Surg [Am]. 1990; 72: 220–229
- Oh, K.-J., Lee, J.W., Kwon, E.T. et al. Comparison of MR imaging findings between extraligamentous and subligamentous disk herniations in the lumbar spine. AJNR. 2013; 34: 683–687
- United States Department of Health and Human Services. Publication no (PHS) 91-1260, International Classification of Diseases Ninth Revision, clinical modification fifth edition, Washington, DC, 1998; Adapted and published by Practice Management Information Corporation, Los Angeles, and by St. Anthony’s Publishing Company, Alexandria, Virginia, 1999.
- Williams, A.L., Haughton, V.M., Daniels, D.L., and Grogan, J.P. Differential CT diagnosis of extruded nucleus pulposus. Radiology. 1983; 148: 141–148
- Modic, M.T. Degenerative disorders of the spine. in: Magnetic resonance imaging of the spine. Yearbook Medical, New York; 1989: 83–95
- Boden, S.D., Davis, D.O., Dina, T.S. et al. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg. 1990; 72: 403–408
- Yu, S., Haughton, V.M., Sether, L.A., and Wagner, M.
Anulus fibrosus in bulging intervertebral disks.Radiology. 1988; 169: 761–763 - Yasuma, T., Makino, E., Saito, S., and Inui, M. Histologic development of intervertebral disc herniation. J Bone Joint Surg. 1986; 68A: 1066–1073
- Sachs, B.L., Vanharanta, H., Spivey, M.A. et al. Dallas discogram description. A new classification of CT/discography in low-back disorders. Spine. 1987; 12: 287–294
- Carragee, E.J., Paragioudakis, S.J., and Khurana, S. Lumbar high-intensity zone and discography in subject without low back problems. Spine. 2000; 25: 2987–2992
- Schellhas, K.P., Pollei, S.R., Gundry, C.R. et al. Lumbar disc high intensity zone. Correlation of magnetic resonance imaging and discography. Spine. 1996; 21: 79–86
- Munter, F.M., Wasserman, B.A., Wu, H.M., and Yousem, D.M. Serial MR imaging of annular tears in lumbar intervertebral disks. Am J Neuroradiol. 2002; 23: 1105–1109
- Quencer, R.M. The abnormal annulus fibrosus: can we infer the acuteness of an annular injury?.Am J Neuroradiol. 2002; 23: 1069
- Czervionke, L.F. Lumbar intervertebral disc disease. Neuroimaging Clin N Am. 1993; : 465–485
- Rothman, S.L.G. and Chafetz, N.I. An anatomic explanation for overreading disc herniations on MRI imaging studies of the lumbar spine: poster presentation. American Society of Neuroradiology,Chicago, Illinois; 1995
- Twomey, L.T. and Taylor, J.R. Age changes in lumbar vertebrae and intervertebral discs. Clin Orthop. 1987; 224: 97–104
- Coventry, M.B., Ghormley, R.K., and Kernohan, J.W. The intervertebral disc: its microscopic anatomy and pathology. (233–7)J Bone Joint Surg. 1945; 27: 105–112
- Farfan, H.F. Mechanical disorders of the low back. Lea & Febiger, ; 1973: 141
- Hirsch, C. and Schajowicz, F. Studies in structural changes in the lumbar annulus fibrosus. Acta Orthop Scand. 1952; 22: 184–231
- Ito, T., Yamada, M., Ikuta, F. et al. Histologic evidence of absorption of sequestration-type herniated disc. Spine. 1996; 21: 230–234
- Liebscher, T., Haefeli, M., Wuertz, K. et al. Age-related variation in cell density of human lumbar intervertebral disc. Spine. 2011; 36: 153–159
- Nathan, H. Osteophytes of the vertebral column. An anatomical study of their development according to age, race, and sex, with consideration as to their etiology and significance. J Bone Joint Surg Am. 1962; 44: 243–268
- Sether, L.A., Yu, S., Haughton, V.M., and Fischer, M.E. Intervertebral disk: normal age-related changes in MR signal intensity. Radiology. 1990; 177: 385–388
- Twomey, L.T. and Taylor, J.R. Age changes in lumbar intervertebral discs. Acta Orthop Scand. 1985;56: 496–499
- Schmorl, G. and Junghanns, H. (American Ed, 1971. Transl. by EF Besemann) (186–98)in: The human spine in health and disease. 2nd. Grune and Stratton, New York; 1971: 141–148
- Pritzker, K.P.H. Aging and degeneration in the lumbar intervertebral disk. Orthop Clin North Am. 1977; 8: 65–77
- Ross, J.S. Babel 2.0. Radiology. 2010; 254: 640–641
- Pfirrmann, C.W., Metzdorf, A., Zanetti, M. et al. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine. 2001; 26: 1873–1878
- Griffith, J.F., Wang, W.X., and Antonio, G.E. Modified Pfirrmann grading system for lumbar intervertebral disc degeneration. Spine. 2007; 32: E708–E712
- Yu, S., Haughton, V.M., Sether, L.A. et al. Criteria for classifying normal and degenerated lumbar intervertebral disks. Radiology. 1989; 170: 323–326
- Brock, M., Patt, S., and Mayer, H.M. The form and structure of the extruded disc. Spine. 1992; 17: 1457–1461
- Williams, A.L. CT diagnosis of degenerative disc disease. The bulging annulus. Radiol Clin North Am. 1983; 21: 289–300
- Masaryk, T.J., Ross, J.S., Modic, M.T. et al. High-resolution MR imaging of sequestered lumbar intervertebral discs. Am J Neuroradiol. 1988; 9: 351–358
- Wiltse, L.L., Berger, P.E., and McCulloch, J.A. A system for reporting the size and location of lesions in the spine. Spine. 1997; 22: 1534–1537
- Saal, J.A., Saal, J.S., and Herzog, R.J. The natural history of lumbar intervertebral disc extrusions treated nonoperatively. Spine. 1990; 15: 683–686
- Fardon DF. Disc nomenclature: current journal practices. Poster presentation, American Orthopaedic Association 110th annual meeting, Boca Raton, FL, 1997.
- Federative Committee on Anatomic Terminology. Terminologia
anatomica . George Thieme Verlag, ; 1998: 27Struttgart

Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.

EXTRA IMPORTANT TOPIC: Sciatica Pain Chiropractic Therapy
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card