


Chiropractor, Dr. Alexander Jimenez discusses a case study in which a chiropractor reports a problem.
This case study isn’t about an athlete. It is all about somebody who works with athletes. Physiotherapists, chiropractors, osteopaths – we all get injured from time to time and we are the worst at getting treatment. We ‘suck it up’ and attempt to handle the issue ourselves. After all, if we can’t fix our own problems, how can we be expected to repair the problems of our clientele? This case study presents an unusual case of neck pain brought on by a seemingly remote problem.
Table of Contents
The Patient
A 35-year-old sports physiotherapist working with a professional rugby team had been suffering with right-sided neck pain for a few months caused by some heavy deadlifts and bench pressing a week before the pain started. He did not seek any treatment from a professional for this issue, as he was self-managing with regular self-releases to his cervical spine, his upper traps and some self ‘Mulligan mobes’ to his cervical spine.
I noticed that he was ‘attending’ to his neck issue a bit so I asked him what the problem was one day. He disclosed that the neck pain had started following a heavy gym session when he had attempted a personal best on the deadlift. Since that day whenever he attempted a deadlift or bench-pressed heavy the ‘nagging’ pain would start up a day or two.
The pain was focused extending down to the point of the joint and starting below the occiput. He noticed some tingling into his forearm and into the underside of his arm. This was sporadic and did not bother him too much.
He described the pain as being a vague stiffness in the neck that would cause him to wake up with a ‘locked’ . He found that although stretching the levator scapulae and self-releases with a trigger ball would give a temporary relief, the pain was a constant low-level ache that would have periods of increased intensity following a gym session that was heavy.
Objective Findings
Upon examination he had a complete range of neck movement but he felt that rotating his head would feel tighter on the right side of his neck. Feeling through his upper trapezius and levator scapulae muscles, it was evident he was holding a lot of muscle tone by means of these muscles in and around those neck muscles. Passive mobilization of his joints on the side, although not painful, did feel hypomobile.
A postural assessment of his scapula position highlighted the scapula was downwardly rotated and also anterior tilted. Based on this I felt that having a feel around his pectoralis minor was warranted and unsurprisingly the pec minor felt hypertonic and tight.
What was also evident was the way he used his right arm and shoulder whilst. Working on elite level players in a hands-on capacity can be a task requiring a lot of muscle contraction through the therapist’s arms and shoulders. Becoming right-handed dominant, whenever he used this arm/hand to work on a participant (massage a tight hamstring, release a tight shoulder muscle, mobilise a stiff lumbar spine or cervical spine) he would unconsciously roll his right shoulder into internal rotation and protract the ideal scapula a lot in comparison with the left side. He was ‘closing’ up the chest space on that right side and generating a habitual shortening of the pec minor muscle.
Probable Cause
With a presentation like this, many causes for the pain may co-exist. The problem may have been focused solely on the tightness and trigger points in the two neck muscles — the levator scapulae and upper trapezius. He had just cause for this to be a problem as the heavy deadlifts can create a ‘traction’ effect due to the force of gravity and weight on the elevator muscles that were scapula.
There was A additional possibility an injury to the right-sided facet joints and/or intervertebral disc. Both these structures can cause referral of pain down the neck and into the shoulder and the history of tingling in the arm could be the result of a nerve root compression at the cervical spine level.
The final possibility was that he suffered from a kind of thoracic outlet syndrome whereby the nerves that pass under the clavicle and through the neck muscles and in addition to the first rib may become compressed due to a downward scapula. I felt this was most unlikely as his feature was muscle pain and more cervical and not the standard symptoms found with thoracic outlet.
These three sources for the neck pain did not fit with me. He had already instigated some self-management to these above muscles; however the pain was still ongoing. And I could not help but think that the combination of the deadlifts, the occupational hazards also and he had to endure the natural position of the scapula led to a tight and hypertonic pectoralis created the problems.
I proposed that the pec minor dragged his scapula into a downwardly rotated position and anterior position that was tilted. My suggestion was that this scapulae position was shortening up the levator scapulae (as it is also a downward rotating muscle of the scapulae) and that this downward rotation was lengthening the upper trapezius (an upward rotator) and creating a lot of passive tension through this muscle. Tension by means of these muscles and trigger points could explain the radiation of pain down through the neck on the tip of the acromian process.
As the levator scapulae attaches to the processes of the cervical spine, a tight and hypertonic muscle may pull down and cause these joints. The little disc and fat pad within the facet joint can then become inflamed and create unilateral neck pain. What’s more, the upper trapezius attaches to the base of tension and the occiput though this muscle will ‘pull’ the head down onto the neck and also increase neck compression through the disc and also place pressure on the facet joints.
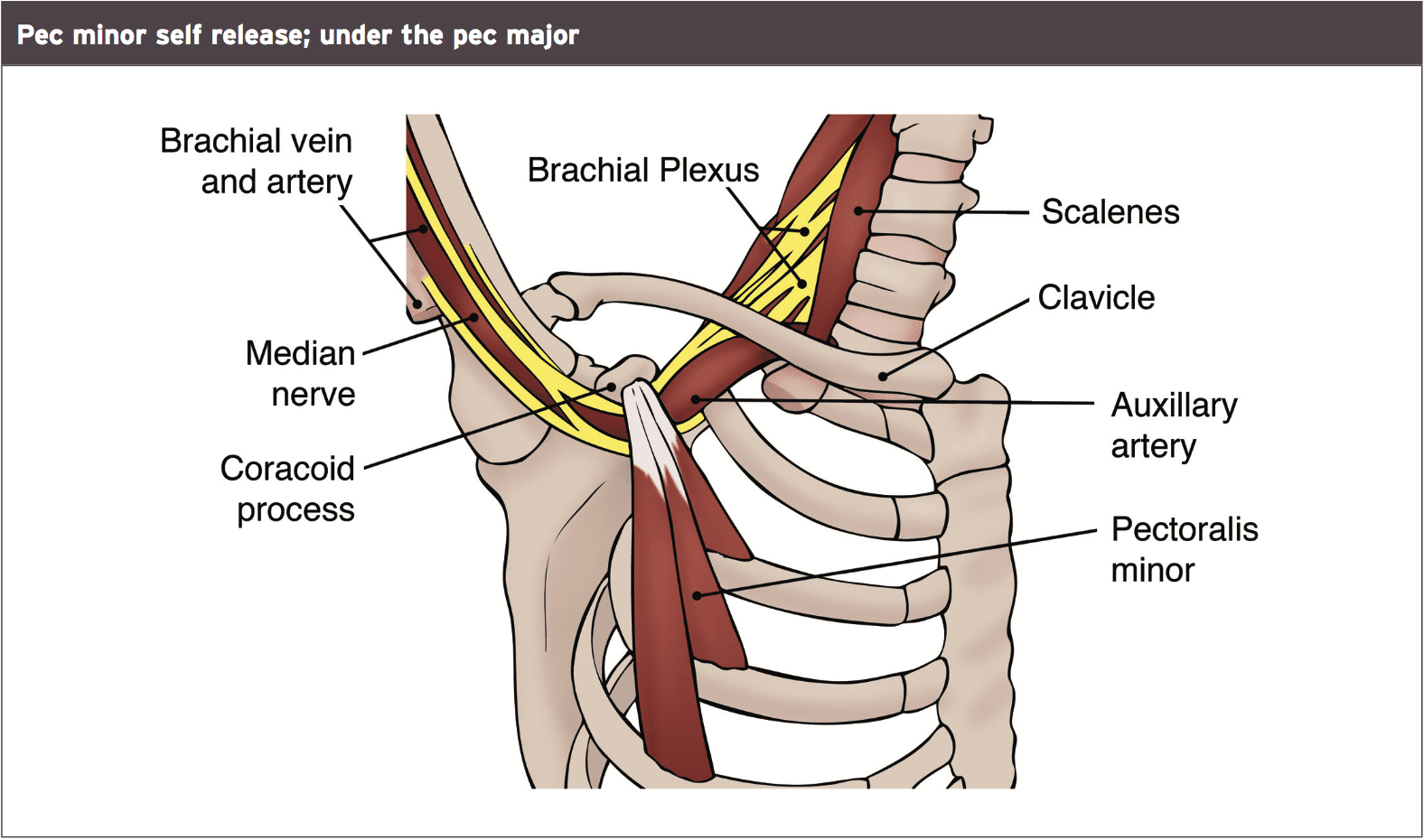
What’s more, the Brachial Plexus (nerve bundle) and some essential arteries and veins run under the pec minor muscle as they course through the chest and migrate down the arm. It was possible that the pec minor, when super- creating and may in reality be pressing on the nerve bundle.
I suggested that heavy deadlifts would exacerbate this problem as the pull of the bar as he deadlifted perpetuate a tight pec minor and possibly would drag the scapular. I also believed that heavy bench pressing would recruit the pec minor to help with the pushing and scapular protraction phase of the bench press.
Therapy
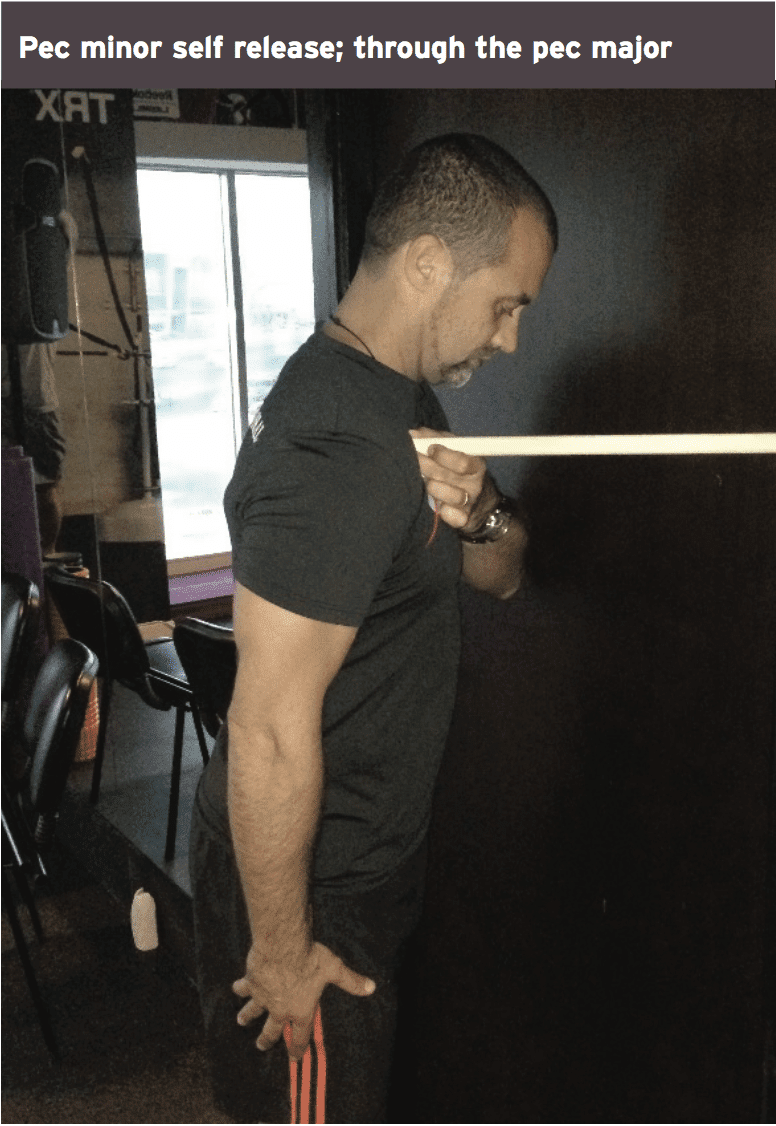
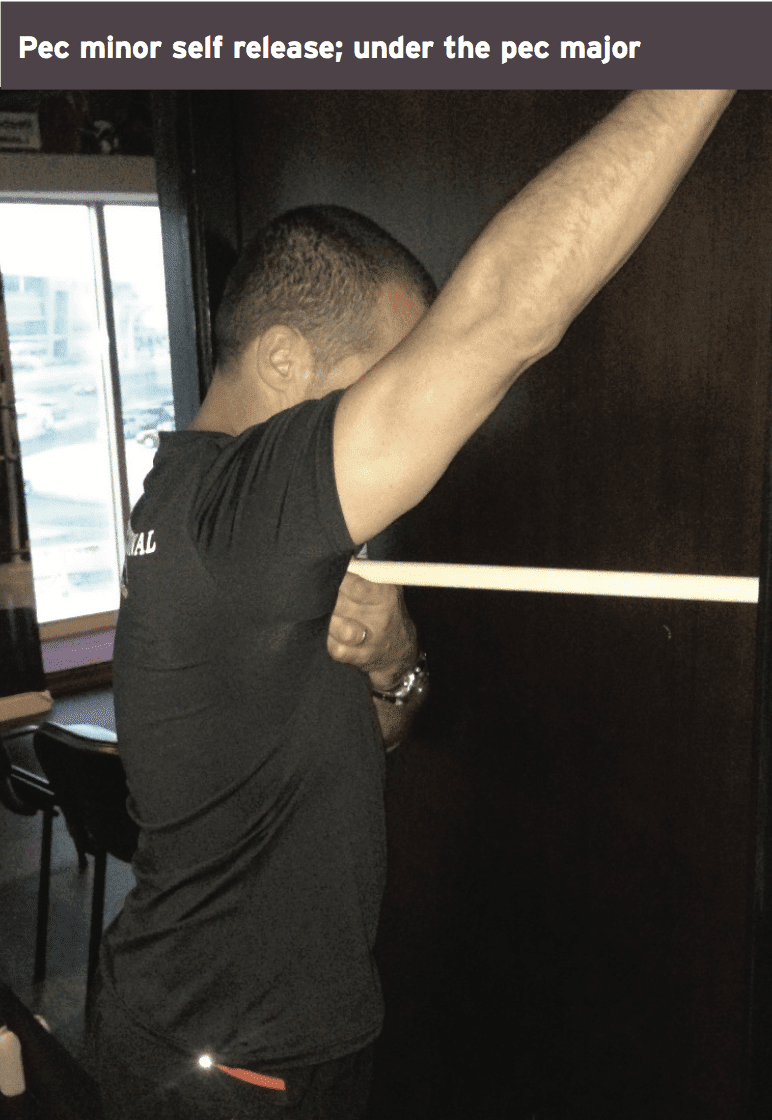
We focused on some deep tissue massage and trigger point releases to the pec minor. This was done in two unique ways. The first way was the approach that is common through the chest wall and pressure directed down onto the pec. The second method was the approach of directly finding the pec minor under the pec major.
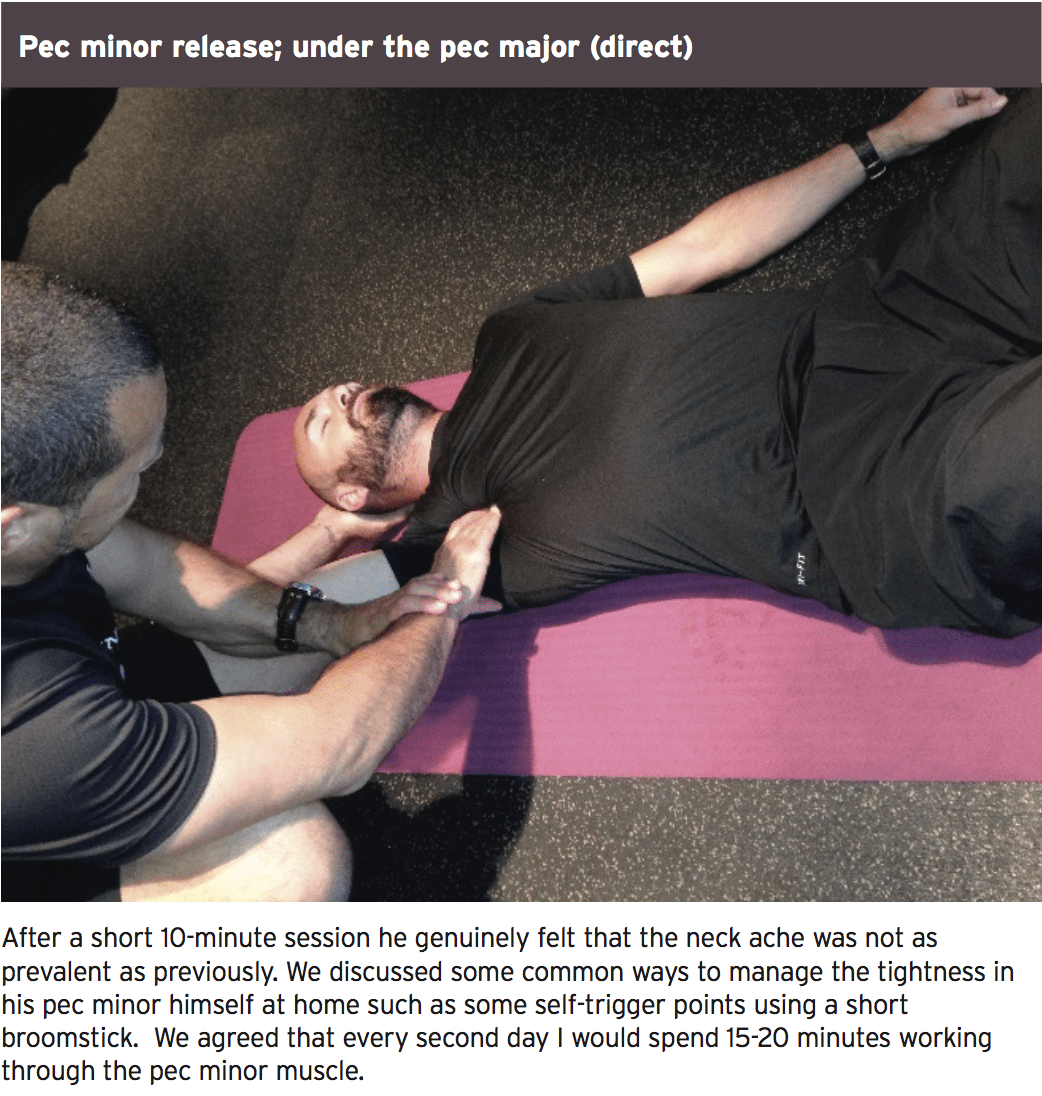
After a short 10-minute session he felt that the neck ache wasn’t as prevalent as previously. We discussed some common tactics to manage the tightness in his pec minor himself at home such as some points utilizing a brief broomstick. We agreed that I would spend 15-20 minutes working through the minor muscle.

 What he had to do was some scapular setting exercises. This consisted of the following steps:
What he had to do was some scapular setting exercises. This consisted of the following steps:
1. Sit in a chair with hands on the lap.
2. Gently tuck the chin in and activate the neck flexor muscles.
3. Gently pull the scapula into retraction position and an upward rotation to activate the trapezius muscle.
4. Hold for 10 seconds. Repeat for 10 repetitions.
The Outcome
He noticed that within 10 days the pain was just a vague awareness in the neck and also the upper trapezius and levator scapulae. He admits that over the course on the upcoming few months the pain had at some point disappeared and he was benching and deadlifting without issues.
Discussion
The pectoralis (pec) minor is a muscle that originates on the anterior rib cage on ribs 3,4,5. It is then directed upwards to insert onto the coracoid process of the scapula. It is a triangular muscle that’s under the pectoralis major and as mentioned above connected with the neurovascular bundle that moves across the chest and into the arm.
 Its functions are to:
Its functions are to:
a. Protract the scapula
b. Depress the scapula
C. the scapula tilts
D. the scapula rotates
e. Work as an accessory muscle during inspiration to open the chest to take in a deep breath. This can only happen if the arms and scapula are fixed and can’t move, like when you place your hands on your hips or on a railing when you are attempting to catch your breath, behind your head.
It’s been implicated in many quadrant pathologies of shoulder, the neck and arm. It’s a muscle that commonly gets very tight, particularly due to habitual use on the dominant side of the body (for most of us right side).
This case study presented a special example of neck pain brought on by a tight pec muscle.
Post Disclaimer
Professional Scope of Practice *
The information herein on "When Chiropractors Have Neck Pain" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Our information scope is limited to Chiropractic, musculoskeletal, physical medicines, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somatovisceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and/or functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and directly or indirectly support our clinical scope of practice.*
Our office has reasonably attempted to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez, DC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, RN*, CCST, IFMCP*, CIFM*, ATN*
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807, New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Florida
Florida License RN License # RN9617241 (Control No. 3558029)
License Compact Status: Multi-State License: Authorized to Practice in 40 States*
Presently Matriculated: ICHS: MSN* FNP (Family Nurse Practitioner Program)
Dr. Alex Jimenez DC, MSACP, RN* CIFM*, IFMCP*, ATN*, CCST
My Digital Business Card