

Migraine Headache Pain Chiropractic Therapy in El Paso, TX

[et_pb_section bb_built=”1″][et_pb_row][et_pb_column type=”4_4″][et_pb_text]
Migraine headaches have been considered to be one of the most frustrating ailments when compared to other common health issues. Generally triggered by stress, the symptoms of migraines, including the debilitating head pain, sensitivity to light and sound as well as the nausea, can tremendously affect a migraineur’s quality of life. However, research studies have found that chiropractic care can help reduce the frequency and the severity of your migraine pain. Many healthcare professionals have demonstrated that a spinal misalignment, or subluxation, may be the source of migraine headache pain. The purpose of the article below is to demonstrate the outcome measures of chiropractic spinal manipulative therapy for migraine.
Table of Contents
Chiropractic Spinal Manipulative Therapy for Migraine: a Three‐Armed, Single‐Blinded, Placebo, Randomized Controlled Trial
Abstract
- Background and purpose: To investigate the efficacy of chiropractic spinal manipulative therapy (CSMT) for migraineurs.
- Methods: This was a prospective three‐armed, single‐blinded, placebo, randomized controlled trial (RCT) of 17 months duration including 104 migraineurs with at least one migraine attack per month. The RCT was conducted at Akershus University Hospital, Oslo, Norway. Active treatment consisted of CSMT, whereas placebo was a sham push manoeuvre of the lateral edge of the scapula and/or the gluteal region. The control group continued their usual pharmacological management. The RCT consisted of a 1‐month run‐in, 3 months intervention and outcome measures at the end of the intervention and at 3, 6 and 12 months follow‐up. The primary end‐point was the number of migraine days per month, whereas secondary end‐points were migraine duration, migraine intensity and headache index, and medicine consumption.
- Results: Migraine days were significantly reduced within all three groups from baseline to post‐treatment (P < 0.001). The effect continued in the CSMT and placebo group at all follow‐up time points, whereas the control group returned to baseline. The reduction in migraine days was not significantly different between the groups (P > 0.025 for interaction). Migraine duration and headache index were reduced significantly more in the CSMT than the control group towards the end of follow‐up (P = 0.02 and P = 0.04 for interaction, respectively). Adverse events were few, mild and transient. Blinding was strongly sustained throughout the RCT.
- Conclusions: It is possible to conduct a manual‐therapy RCT with concealed placebo. The effect of CSMT observed in our study is probably due to a placebo response.
- Keywords: chiropractic, headache, migraine, randomized controlled trial, spinal manipulative therapy

Dr. Alex Jimenez’s Insight
Neck pain and headaches are the third most common reason people seek chiropractic care. Many research studies have demonstrated that chiropractic spinal manipulative therapy is a safe and effective alternative treatment option for migraines. Chiropractic care can carefully correct any spinal misalignment, or subluxation, found along the length of the spine, which has been shown to be a source for migraine headaches. In addition, spinal adjustments and manual manipulations can help reduce stress and muscle tension by decreasing the amount of pressure being placed against the complex structures of the spine as a result of a spinal misalignment, or subluxation. By realigning the spine as well as reducing stress and muscle tension, chiropractic care can improve migraine symptoms and decrease their frequency.
Introduction
The socio‐economic costs of migraine are enormous due to its high prevalence and disability during attacks [1, 2, 3]. Acute pharmacological treatment is usually the first treatment option for migraine in adults. Migraineurs with frequent attacks, insufficient effect and/or contraindication to acute medication are potential candidates for prophylactic treatment. Migraine prophylactic treatment is often pharmacological, but manual therapy is not unusual, especially if pharmacological treatment fails or if the patient wishes to avoid medicine [4]. Research has suggested that spinal manipulative therapy may stimulate neural inhibitory systems at different spinal cord levels because it might activate various central descending inhibitory pathways [5, 6, 7, 8, 9, 10].
Pharmacological randomized controlled trials (RCTs) are usually double‐blinded, but this is not possible in manual‐therapy RCTs, as the interventional therapist cannot be blinded. At present there is no consensus on a sham procedure in manual‐therapy RCTs that mimics placebo in pharmacological RCTs [11]. Lack of a proper sham procedure is a major limitation in all previous manual‐therapy RCTs [12, 13]. Recently, we developed a sham chiropractic spinal manipulative therapy (CSMT) procedure, where participants with migraine were unable to distinguish between real and sham CSMT evaluated after each of 12 individual interventions over a 3‐month period [14].
The first objective of this study was to conduct a manual‐therapy three‐armed, single‐blinded, placebo RCT for migraineurs with a methodological standard similar to that of pharmacological RCTs.
The second objective was to assess the efficacy of CSMT versus sham manipulation (placebo) and CSMT versus controls, i.e. participants who continued their usual pharmacological management.
Methods
Study Design
The study was a three‐armed, single‐blinded, placebo RCT over 17 months. The RCT consisted of a 1‐month baseline, 12 treatment sessions over 3 months with follow‐up measures at the end of intervention, 3, 6 and 12 months later.
Participants were, before baseline, randomized equally into three groups: CSMT, placebo (sham manipulation) and control (continued their usual pharmacological management).
The design of the study conformed to the recommendations of the International Headache Society (IHS) and CONSORT (Appendix S1) [1, 15, 16]. The Norwegian Regional Committee for Medical Research Ethics and the Norwegian Social Science Data Services approved the project. The RCT was registered at ClinicalTrials.gov (ID no: NCT01741714). The full trial protocol has been published previously [17].
Participants
Participants were recruited from January to September 2013 primarily through the Department of Neurology, Akershus University Hospital. Some participants were also recruited through General Practitioners from Akershus and Oslo Counties or media advertisement. All participants received posted information about the project followed by a telephone interview.
Eligible participants were migraineurs of 18–70 years old with at least one migraine attack per month and were allowed to have concomitant tension‐type headache but no other primary headaches. All participants were diagnosed by a chiropractor with experience in headache diagnostics during the interview and according to the International Classification of Headache Disorders‐II (ICHD‐II) 2. A neurologist had diagnosed all migraineurs from Akershus University Hospital.
Exclusion criteria were contraindication to spinal manipulative therapy, spinal radiculopathy, pregnancy, depression and CSMT within the previous 12 months. Participants who received manual therapy [18], changed their prophylactic migraine medicine or became pregnant during the RCT were informed that they would be withdrawn from the study at that time and regarded as drop‐outs. Participants were allowed to continue and change acute migraine medication throughout the study period.
Eligible participants were invited to an interview and physical assessment including meticulous spinal column investigation by a chiropractor (A.C.). Participants randomized to the CSMT or the placebo group had a full spine radiographic examination.
Randomization and Masking
After written consent was obtained, participants were equally randomized into one of the three study arms by drawing one single lot. Numbered sealed lots with the three study arms were each subdivided into four subgroups by age and gender, i.e. 18–39 or 40–70 years, and men or women.
After each treatment session, the participants in the CSMT and the placebo group completed a questionnaire on whether they believed CSMT treatment was received, and how certain they were that active treatment was received on a 0–10 numeric rating scale, where 10 represented absolute certainty [14].
Both the block randomization and the blinding questionnaire were exclusively administered by a single external party.
Interventions
The CSMT group received spinal manipulative therapy using the Gonstead method, a specific contact, high‐velocity, low‐amplitude, short‐lever spinal with no post‐adjustment recoil that was directed to spinal biomechanical dysfunction (full spine approach) as diagnosed by standard chiropractic tests at each individual treatment session [19].
The placebo group received sham manipulation, a broad non‐specific contact, low‐velocity, low‐amplitude sham push manoeuvre in a non‐intentional and non‐therapeutic directional line of the lateral edge of the scapula and/or the gluteal region [14]. All of the non‐therapeutic contacts were performed outside the spinal column with adequate joint slack and without soft tissue pre‐tension so that no joint cavitations occurred. The sham manipulation alternatives were pre‐set and equally interchanged among the placebo participants according to protocol during the 12‐week treatment period to strengthen the study validity. The placebo procedure is described in detail in the available trial protocol [17].
Each intervention session lasted for 15 min and both groups underwent the same structural and motion assessments prior to and after each intervention. No other intervention or advice was given to participants during the trial period. Both groups received interventions at Akershus University Hospital by a single experienced chiropractor (A.C.).
The control group continued their usual pharmacological management without receiving manual intervention by the clinical investigator.
Outcomes
The participants filled in a validated diagnostic headache diary throughout the study and returned them on a monthly basis [20]. In the case of unreturned diaries or missing data, the participants were contacted by phone to secure compliance.
The primary end‐point was number of migraine days per month (30 days/month). At least 25% reduction of migraine days from baseline to end of intervention, with the same level maintained at 3, 6 and 12 months follow‐up was expected in the CSMT group.
Secondary end‐points were migraine duration, migraine intensity and headache index (HI), and medicine consumption. At least 25% reduction in duration, intensity and HI, and at least 50% reduction in medicine consumption were expected from baseline to end of intervention, with the same level maintained at 3, 6 and 12 months follow‐up in the CSMT group.
No change was expected for primary and secondary end‐point in the placebo and the control group.
A migraine day was defined as a day on which migraine with aura, migraine without aura or probable migraine occurred. Migraine attacks lasting for >24 h were calculated as one attack unless pain‐free intervals of ≥48 h had occurred [21]. If a patient fell asleep during a migraine attack and woke up without a migraine, in accordance with the ICHD‐III β, the duration of the attack was recorded as persisting until the time of awakening [22]. The minimum duration of a migraine attack was 4 h unless a triptan or drug containing ergotamine was used, in which case we specified no minimum duration. HI was calculated as mean migraine days per month (30 days) × mean migraine duration (h/day) × mean intensity (0–10 numeric rating scale).
The primary and secondary end‐points were chosen based on the Task Force of the IHS Clinical Trial Subcommittee’s clinical trial guidelines [1, 15]. Based on previous reviews on migraine, a 25% reduction was considered to be a conservative estimate [12, 13].
The outcome analyses were calculated during the 30 days after the last intervention session and 30 days after the follow‐up time points, i.e. 3, 6 and 12 months, respectively.
All adverse events (AEs) were recorded after each intervention in accordance with the recommendations of CONSORT and the IHS Task Force on AEs in migraine trials [16, 23].
Statistical Analysis
We based the power calculation on a recent study of topiramate in migraineurs [24]. We hypothesized the average difference in reduction of number of migraine days per month between the active and the placebo, and between the active and the control groups of 2.5 days, with SD of 2.5 for reduction in each group. As primary analysis includes two group comparisons, the significance level was set at 0.025. For the power of 80%, a sample size of 20 patients was required in each group to detect a significant difference in reduction of 2.5 days.
Patient characteristics at baseline were presented as means and SD or frequencies and percentages in each group and compared by independent samples t‐test and χ 2 test.
Time profiles of all end‐points were compared between the groups. Due to repeated measurements for each patient, linear mixed models accounting for the intra‐individual variations were estimated for all end‐points. Fixed effects for (non‐linear) time, group allocation and interaction between the two were included. Random effects for patients and slopes were entered into the model. As the residuals were skewed, the bootstrap inference based on 1000 cluster samples was used. Pairwise comparisons were performed by deriving individual time point contrasts within each group at each time point with the corresponding P‐values and 95% confidence intervals. Medicine consumption within groups was reported by mean doses with SD, and groups were compared by an independent samples median test. A dose was defined as a single administration of a triptan or ergotamine; paracetamol 1000 mg ± codeine; non‐steroidal anti‐inflammatory drugs (tolfenamic acid, 200 mg; diclofenac, 50 mg; aspirin, 1000 mg; ibuprofen, 600 mg; naproxen, 500 mg); and morphinomimetics (tramadol, 50 mg). None of the patients changed study arm and none of the drop‐outs filled in headache diaries after withdrawal from the study. Hence, only per protocol analysis was relevant.
The analyses were blinded to treatment allocation and conducted in SPSS v22 (IBM Corporation, Armonk, NY, USA) and STATA v14 (JSB) (StataCorp LP, College Station, TX, USA). A significance level of 0.025 was applied for the primary end‐point, whereas elsewhere a level of 0.05 was used.
Ethics
Good clinical practice guidelines were followed [25]. Oral and written information about the project was provided in advance of inclusion and group allocation. Written consent was obtained from all participants. Participants in the placebo and control group were promised CSMT treatment after the RCT, if the active intervention was found to be effective. Insurance was provided through the Norwegian System of Compensation to Patients (Patient Injury Compensation), an independent national body that compensates patients injured by treatments provided by the Norwegian health service. A stopping rule was defined for withdrawing participants from this study in accordance with the recommendations in the CONSORT extension for Better Reporting of Harms [26]. All AEs were monitored during the intervention period and acted on as they occurred according to the recommendations of CONSORT and the IHS Task Force on AEs in migraine trials [16, 23]. In case of severe AE, the participant would be withdrawn from the study and referred to the General Practitioner or hospital emergency department depending on the event. The investigator (A.C.) was available by mobile phone at any time throughout the study treatment period.
Results
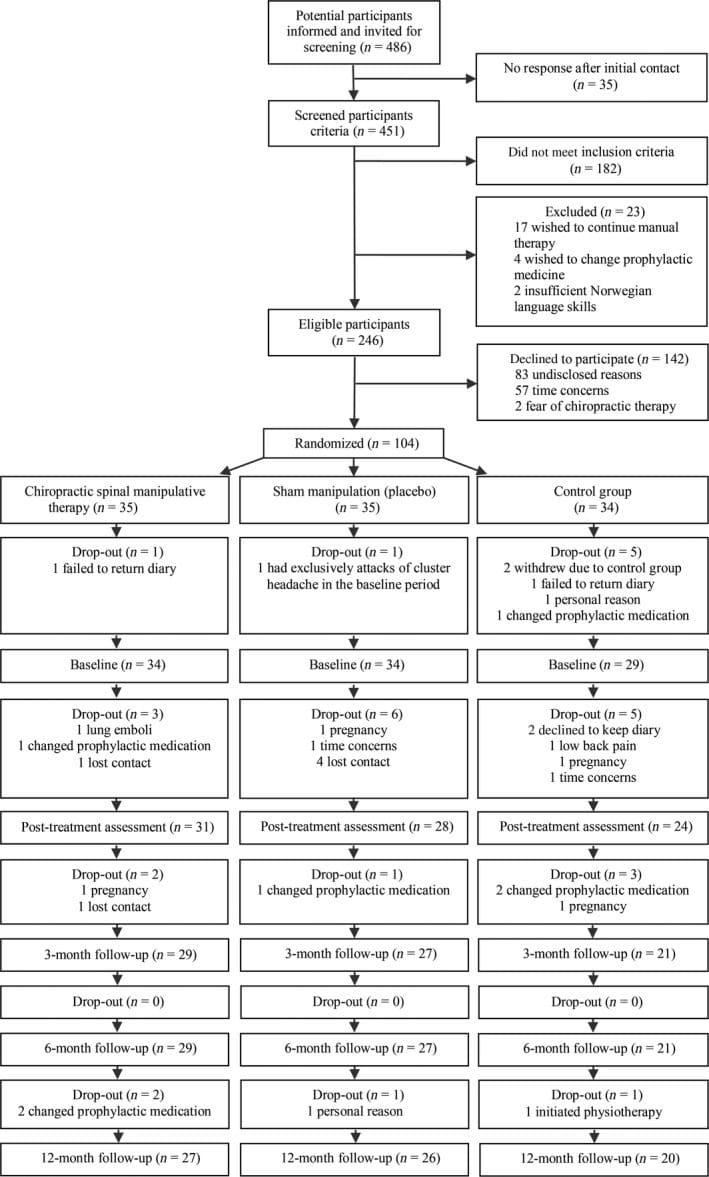
Figure 1 shows a flow chart of the 104 migraineurs included in the study. Baseline and demographic characteristics were similar across the three groups (Table 1).

Outcome Measures
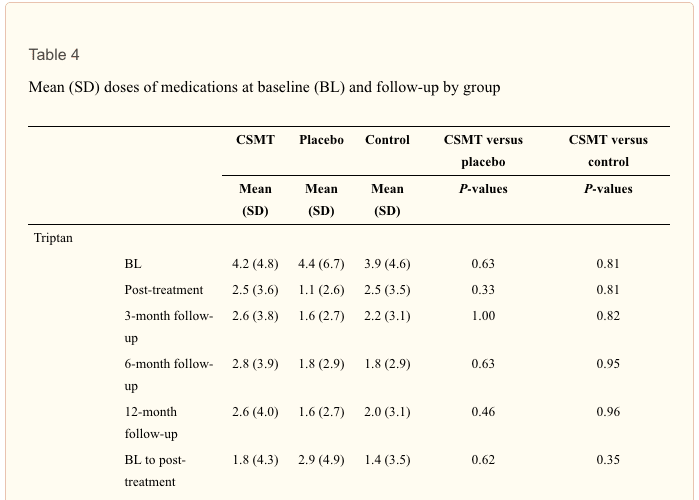
The results on all end‐points are presented in Fig. 2a–d and Tables 2, 3, 4.
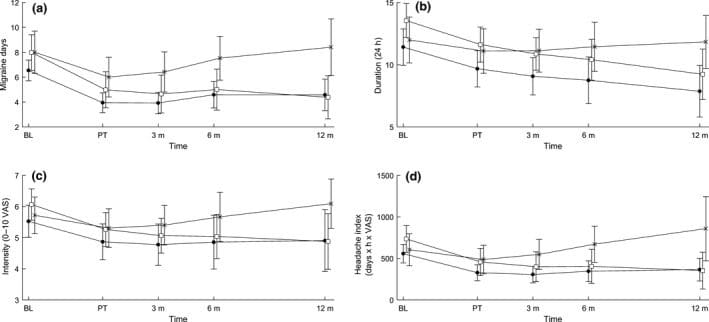
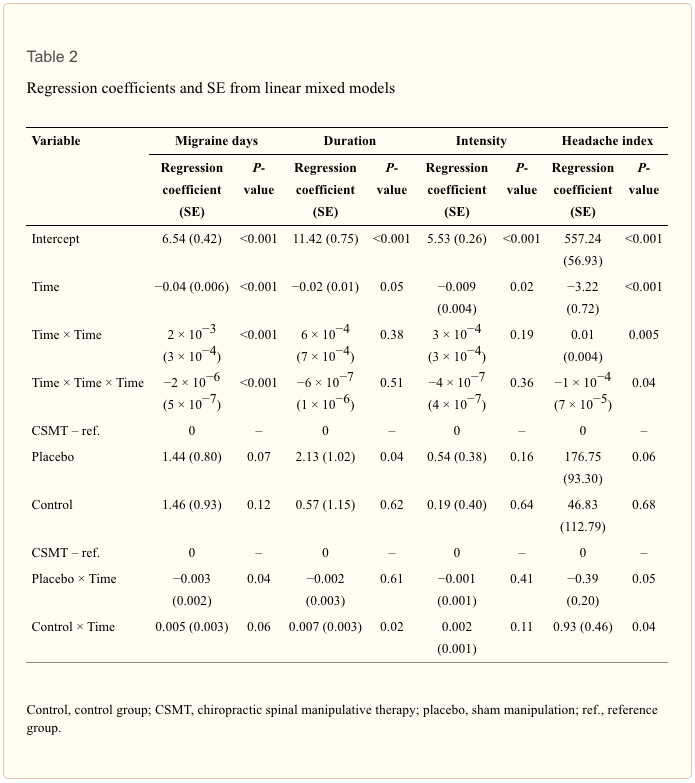
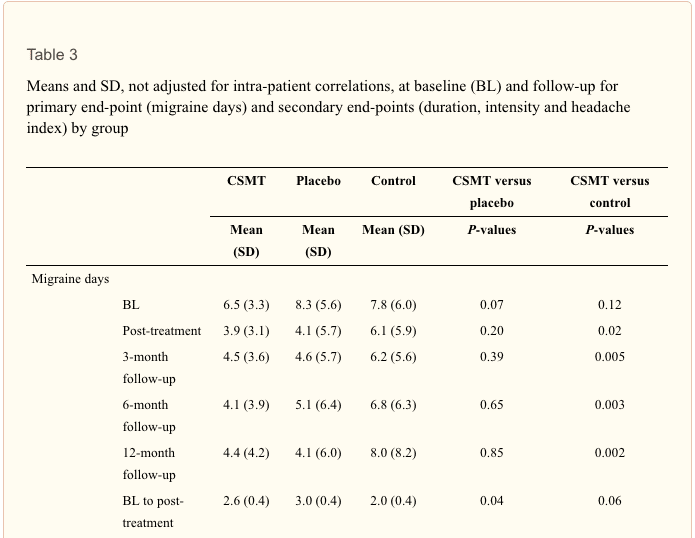
Primary end‐point. Migraine days were significantly reduced within all groups from baseline to post‐treatment (P < 0.001). The effect continued in the CSMT and the placebo groups at 3, 6 and 12 months follow‐up, whereas migraine days reverted to baseline level in the control group (Fig. 2a). The linear mixed model showed no overall significant differences in change in migraine days between the CSMT and the placebo groups (P = 0.04) or between the CSMT and the control group (P = 0.06; Table 2). However, the pairwise comparisons at individual time points showed significant differences between the CSMT and the control group at all time points starting at post‐treatment (Table 3).
Secondary end‐points. There was a significant reduction from baseline to post‐treatment in migraine duration, intensity and HI in the CSMT (P = 0.003, P = 0.002 and P < 0.001, respectively) and the placebo (P < 0.001, P = 0.001 and P < 0.001, respectively) groups, and the effect continued at 3, 6 and 12 months follow‐up.
The only significant differences between the CSMT and control groups were change in migraine duration (P = 0.02) and in HI (P = 0.04; Table 2).
At 12 months follow‐up, change in consumption of paracetamol was significantly lower in the CSMT group as compared with the placebo (P = 0.04) and control (P = 0.03) groups (Table 4).
Blinding. After each of the 12 intervention sessions, >80% of the participants believed they had received CSMT regardless of group allocation. The odds ratio for believing that CSMT treatment was received was >10 at all treatment sessions in both groups (all P < 0.001).
Adverse effects. A total of 703 of the potential 770 intervention sessions were assessed for AEs (355 in the CSMT group and 348 in the placebo group). Reasons for missed AE assessment were drop‐out or missed intervention sessions. AEs were significantly more frequent in the CSMT than the placebo intervention sessions (83/355 vs. 32/348; P < 0.001). Local tenderness was the most common AE reported by 11.3% (95% CI, 8.4–15.0) in the CSMT group and 6.9% (95% CI, 4.7–10.1) in the placebo group, whereas tiredness on the intervention day and neck pain were reported by 8.5% and 2.0% (95% CI, 6.0–11.8 and 1.0–4.0), and 1.4% and 0.3% (95% CI, 0.6–3.3 and 0.1–1.9), respectively. All other AEs (lower back pain, face numbness, nausea, provoked migraine attack and fatigue in arms) were rare (<1%). No severe or serious AEs were reported.
Discussion
To our knowledge, this is the first manual‐therapy RCT with a documented successful blinding. Our three‐armed, single‐blinded, placebo RCT evaluated the efficacy of CSMT in the treatment of migraine versus placebo (sham chiropractic) and control (usual pharmacological treatment). The results showed that migraine days were significantly reduced within all three groups from baseline to post‐treatment. The effect continued in the CSMT and placebo groups at all follow‐up time points, whereas the control group returned to baseline. AEs were mild and transient, which is in accordance with previous studies.
The study design adhered to the recommendations for pharmacological RCTs as given by the IHS and CONSORT [1, 15, 16]. Manual‐therapy RCTs have three major obstacles as compared with pharmacological RCTs. Firstly, it is impossible to blind the investigator in relation to the applied treatment. Secondly, consensus on an inert placebo treatment is lacking [11]. Thirdly, previous attempts to include a placebo group have omitted validating the blinding, thus, it remains unknown whether active and placebo treatment were concealed [27]. Due to these challenges we decided to conduct a three‐armed, single‐blinded RCT, which also included a control group that continued usual pharmacological treatment in order to obtain an indication of the magnitude of the placebo response.
It has been suggested that, in pharmacological double‐blind placebo RCTs, only 50% will believe that they receive active treatment in each group, if the blinding is perfect. However, this may not be true in manual‐therapy RCTs, because the active and placebo physical stimulus might be more convincing than a tablet [28]. A single investigator reduces inter‐investigator variability by providing similar information to all participants and it is generally recommended that the placebo intervention should resemble the active treatment in terms of procedure, treatment frequency and time spent with the investigator to allow for similar expectations in both groups [28]. The importance of our successful blinding is emphasized by the fact that all previous manual‐therapy RCTs on headache lack placebo. Thus, we believe that our results discussed below are valid at the same level as a pharmacological RCT [14].
Prospective data are more reliable than retrospective data in terms of recall bias; however, non‐compliance can be a challenge, especially at the end of the study. We believe the frequent contact between participants and the investigator, including monthly contact in the follow‐up period, probably maintained high compliance throughout our study.
Although our study sample ended with 104 participants in the three groups, the power calculation assumption and the high completion rate support the data achieved being valid for the investigated population. The Gonstead method is used by 59% of chiropractors [19] and, thus, the results are generalizable for the profession. Diagnostic certainty is one of our major strengths as nearly all of the participants had been diagnosed by a neurologist according to the ICHD‐II [2]. In contrast to previous chiropractic migraine RCTs that recruited participants through media such as newspapers and radio advertisement [12], the majority of our participants were recruited from the Department of Neurology, Akershus University Hospital, indicating that the migraineurs may have more frequent/severe attacks that are difficult to treat than the general population, as they were referred by their General Practitioner and/or practicing neurologist. Thus, our study is representative of primarily the tertiary clinic population, and the outcome might have been different if participants had been recruited from the general population. The percentage of neck pain has been found to be high in patients with migraine [29] and, thus, the high percentage of non‐radicular spinal pain in our study might be a confounder for which effect was seen on migraine days.
Three pragmatic chiropractic manual‐therapy RCTs using the diversified technique have previously been conducted for migraineurs [12, 30, 31, 32]. An Australian RCT showed within‐group reduction in migraine frequency, duration and intensity of 40%, 43% and 36%, respectively, at 2 months follow‐up [30]. An American study found migraine frequency and intensity to reduce within‐group by 33% and 42%, respectively, at 1 month follow‐up [31]. Another Australian study, which was the only RCT to include a control group, i.e. detuned ultrasound, found a within‐group reduction of migraine frequency and duration of 35% and 40%, respectively, at 2 months follow‐up in the CSMT group, as compared with a within‐group reduction of 17% and 20% in the control group, respectively [32]. The reduction in migraine days was similar to ours (40%) in the CSMT group from baseline to 3 months follow‐up, whereas migraine duration and intensity were less reduced at 3 months follow‐up, i.e. 21% and 14%, respectively. Long‐term follow‐up comparisons are impossible as neither of the previous studies included a sufficient follow‐up period. Our study design including strong internal validity allows us to interpret the effect seen as a placebo response.
Our RCT had fewer AEs as compared with previous manual‐therapy studies, but of similar transient and mild character [33, 34, 35, 36, 37, 38, 39]. However, it was not sufficiently powered to detect uncommon serious AEs. In comparison, AEs in pharmacological migraine prophylactic placebo RCTs are common including non‐mild and non‐transient AEs [40, 41].
Conclusion
The blinding was strongly sustained throughout the RCT, AEs were few and mild, and the effect in the CSMT and placebo group was probably a placebo response. Because some migraineurs do not tolerate medication because of AEs or co‐morbid disorders, CSMT might be considered in situations where other therapeutic options are ineffective or poorly tolerated.
Disclosure of Conflicts of Interest
All authors have completed the International Committee of Medical Journal Editors uniform disclosure form and declare no financial or other conflicts of interest.
Supporting Information
Ncbi.nlm.nih.gov/pmc/articles/PMC5214068/#ene13166-tbl-0001
Acknowledgements
The authors want to express their sincere gratitude to Akershus University Hospital, which kindly provided the research facilities, and Chiropractor Clinic 1, Oslo, Norway, which performed all x‐ray assessments. This study was supported by grants from Extrastiftelsen, the Norwegian Chiropractic Association, Akershus University Hospital and University of Oslo in Norway.
In conclusion, the debilitating symptoms of migraines, including the severe head pain and the sensitivity to light and sound as well as the nausea, can affect an individual’s quality of life, fortunately, chiropractic care has been demonstrated to be a safe and effective treatment option for migraine headache pain. Furthermore, the article above demonstrated that migraineurs experienced reduced symptoms and migraine days as a result of chiropractic care. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez

Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.

EXTRA IMPORTANT TOPIC: Neck Pain Treatment El Paso, TX Chiropractor
MORE TOPICS: EXTRA EXTRA: El Paso, Tx | Athletes
[/et_pb_text][et_pb_accordion _builder_version=”3.0.106″][et_pb_accordion_item _builder_version=”3.0.106″ title=”Blank” use_background_color_gradient=”off” background_color_gradient_start=”#2b87da” background_color_gradient_end=”#29c4a9″ background_color_gradient_type=”linear” background_color_gradient_direction=”180deg” background_color_gradient_direction_radial=”center” background_color_gradient_start_position=”0%” background_color_gradient_end_position=”100%” background_color_gradient_overlays_image=”off” parallax=”off” parallax_method=”on” background_size=”cover” background_position=”center” background_repeat=”no-repeat” background_blend=”normal” allow_player_pause=”off” background_video_pause_outside_viewport=”on” text_shadow_style=”none” box_shadow_style=”none” custom_css_main_element=”display:none;” /][et_pb_accordion_item _builder_version=”3.0.106″ title=”References” use_background_color_gradient=”off” background_color_gradient_start=”#2b87da” background_color_gradient_end=”#29c4a9″ background_color_gradient_type=”linear” background_color_gradient_direction=”180deg” background_color_gradient_direction_radial=”center” background_color_gradient_start_position=”0%” background_color_gradient_end_position=”100%” background_color_gradient_overlays_image=”off” parallax=”off” parallax_method=”on” background_size=”cover” background_position=”center” background_repeat=”no-repeat” background_blend=”normal” allow_player_pause=”off” background_video_pause_outside_viewport=”on” text_shadow_style=”none” box_shadow_style=”none”]
[/et_pb_accordion_item][et_pb_accordion_item _builder_version=”3.0.106″ title=”Close Accordion” use_background_color_gradient=”off” background_color_gradient_start=”#2b87da” background_color_gradient_end=”#29c4a9″ background_color_gradient_type=”linear” background_color_gradient_direction=”180deg” background_color_gradient_direction_radial=”center” background_color_gradient_start_position=”0%” background_color_gradient_end_position=”100%” background_color_gradient_overlays_image=”off” parallax=”off” parallax_method=”on” background_size=”cover” background_position=”center” background_repeat=”no-repeat” background_blend=”normal” allow_player_pause=”off” background_video_pause_outside_viewport=”on” open_toggle_background_color=”#ffffff” closed_toggle_background_color=”#ffffff” text_shadow_style=”none” custom_padding=”0px|||” custom_padding_tablet=”0px|||” custom_padding_phone=”0px|||” box_shadow_style=”none” custom_css_main_element=”border:none;” custom_css_toggle_title=”font-size:0.8em;” custom_css_toggle_icon=”display:none;” /][/et_pb_accordion][/et_pb_column][/et_pb_row][/et_pb_section]
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Comments are closed.