

Effectiveness of Mindfulness on Herniated Discs & Sciatica in El Paso, TX
[et_pb_section bb_built=”1″][et_pb_row][et_pb_column type=”4_4″][et_pb_text]
Chronic low back pain is the second most common cause of disability in the United States. Approximately 80 percent of the population will experience back pain at least once throughout their lifetime. The most prevalent causes of chronic low back pain include: herniated discs, sciatica, injuries from lifting heavy objects or any other non-specific spine injury. However, people will often react differently to their symptoms. These differing responses are due to people’s psychological attitudes and outlooks.
Table of Contents
Chronic Low Back Pain and the Mind
Stress has been associated with increased pain but your own personal health beliefs and coping strategies can influence your own perception of pain as well. That’s because psychological vulnerabilities can alter your brain and intensify the pain. Additionally, the pain itself can rewire the brain. When pain first occurs, it impacts the pain-sensitivity brain circuits. When pain becomes persistent, the associated brain activity switches from the pain circuits to circuits that process emotions. That’s why it’s believed that stress, anxiety and depression can cause as well as worsen chronic low back pain.
Managing the Scourge of Chronic Low Back Pain
Fortunately, several stress management methods and techniques can help improve chronic low back pain. Mindfulness is the most common treatment with the best supporting evidence towards improving and managing chronic pain. A recent study demonstrated that mindfulness-based stress reduction, or MBSR, including mindfulness meditation and other mindfulness interventions, can help reduce back pain and enhance psychological control by increasing brain blood flow to the frontal lobe. Practicing mindfulness involves activating a brain relaxation pathway by intentionally ignoring mental “chatter” and focusing on your breathing. Cognitive behavioral therapy, or CBT can also be helpful for chronic low back pain. Cognitive behavioral therapy can prevent an acute injury from progressing to chronic low back pain. Hypnosis may also help relieve chronic low back pain. However, CBT and hypnosis have weaker evidence to support their effectiveness on back pain.
Mind Over Matter
So while it may seem that chronic low back pain is all “in your head”, research studies have demonstrated that stress can influence painful symptoms. “Mind” includes “matter,” especially when you consider that the physical “matter” of the brain plays a major role in mindset changes. This is especially true when it comes to the brain-based changes related to low back pain. The purpose of the article below is to demonstrate the effectiveness of mindfulness meditation on chronic low back pain.
Effectiveness of Mindfulness Meditation on Pain and Quality of Life of Patients with Chronic Low Back Pain
Abstract
- Background and aim: Recovery of patients with chronic low back pain (LBP) is depended on several physical and psychological factors. Therefore, the authors aimed to examine the efficacy of mindfulness based stress reduction (MBSR) as a mind-body intervention on quality of life and pain severity of female patients with nonspecific chronic LBP (NSCLBP).
- Methods: Eighty-eight patients diagnosed as NSCLBP by physician and randomly assigned to experimental (MBSR+ usual medical care) and the control group (usual medical care only). The subjects assessed in 3 times frames; before, after and 4 weeks after intervention by Mac Gil pain and standard brief quality of life scales. Data obtained from the final sample analyzed by ANCOVA using SPSS software.
- Results: The findings showed MBSR was effective in reduction of pain severity and the patients who practiced 8 sessions meditation reported significantly lower pain than patients who only received usual medical care. There was a significant effect of the between subject factor group (F [1, 45] = 16.45, P < 0.001) and (F [1, 45] = 21.51, P < 0.001) for physical quality of life and (F [1, 45] = 13.80, P < 0.001) and (F [1, 45] = 25.07, P < 0.001) mental quality of life respectively.
- Conclusion: MBSR as a mind-body therapy including body scan, sitting and walking meditation was effective intervention on reduction of pain severity and improvement of physical and mental quality of life of female patients with NSCLBP.
- Keywords: Chronic low back pain, mindfulness based stress reduction, pain, quality of life, SF-12
Introduction
In nonspecific low back pain (NSLBP) the pain is not related to conditions such as fractures, spondylitis, direct trauma, or neoplastic, infectious, vascular, metabolic, or endocrine-related although it is a cause of limitation in daily activities due to actual pain or fear of pain.[1] Unfortunately, the majority of LBP patients (80–90%) suffers from nonspecific LBP which leads to considerable pain-related disability and limitation in daily activities.[1,2] Chronic LBP is not only prevalent, but is also a source of great physical disability, role impairment, and diminished psychological well-being and quality of life.[1]
Prior to the current accepted biopsychosocial model, the biomedical model dominated all illness conceptualizations for almost 300 years and still dominates in the popular imagination. First proposed by Engel (1977) the biopsychosocial model acknowledges biological processes but also highlights the importance of experiential and psychological factors in pain. The famous gate control theory of pain[3] also proposed that the brain plays a dynamic role in pain perception as opposed to being a passive recipient of pain signals. They suggested psychological factors can inhibit or enhance sensory flow of pain signals and thus influence the way brain ultimately responds to painful stimulation.[4] If mind processes can change the way the brain processes pain then this holds tremendous potential for psychological intervention to produce reduced pain signals from the brain.
Kabat-Zinn’s et al. (1986) described the process of pain reduction in his paper on mindfulness and meditation. The process of pain reduction occurred by “an attitude of detached observation toward a sensation when it becomes prominent in the field of awareness and to observe with similar detachment the accompanying but independent cognitive processes which lead to evaluation and labeling of the sensation as painful, as hurt.” Thus, by “uncoupling” the physical sensation, from the emotional and cognitive experience of pain, the patient is able to reduce the pain.[5] The patients’ descriptions of distraction from pain, identifying maladaptive coping strategies toward pain and heightened awareness of pain sensation leading to behavioral changes are examples of how pain is unassociated with emotion, cognition, and sensation [Figure 1]. Therefore recently these theories attracted several researchers who are working on pain.
Mindfulness meditation has roots in Buddhist Vipassana philosophy and practice and has been independently adopted within clinical psychology in Western societies.[6,7,8,9] Recently in Netherlands Veehof et al. conducted a systematic review of controlled and noncontrolled studies on effectiveness of acceptance-based interventions such as mindfulness-based stress reduction program, acceptance and commitment therapy for chronic pain. Primary outcomes measured were pain intensity and depression. Secondary outcomes measured were anxiety, physical well-being and quality of life.[10] Twenty-two studies randomized controlled studies clinical controlled studies without randomization and noncontrolled studies were included totaling 1235 patients with chronic pain. An effect size on pain of (0.37) was found in the controlled studies. The effect on depression was (0.32). The authors concluded that ACT and mindfulness interventions had similar effects to other cognitive-behavioral therapy interventions and that these types of interventions may be a useful alternative or adjunct to current therapies. Chiesa and Serretti also conducted another systematic review on 10 mindfulness interventions.[11] The main findings were that these interventions produced small nonspecific effects in terms of reducing chronic pain and symptoms of depression. When compared to active control groups (support and education) no additional significant effects were noted.
In summary, there is a need for further studies into the specific effects of mindfulness studies on chronic pain. Regarding as the researcher knowledge efficacy of mindfulness has not been explored on quality of life of chronic pain patients in Iran. The authors aimed to examine the impact of mindfulness based stress reduction (MBSR) protocol designed for pain management on quality of life and pain of a homogeneous sample of females with nonspecific chronic LBP (NSCLBP) in comparison of the usual medical care group.
Methods
Sampling
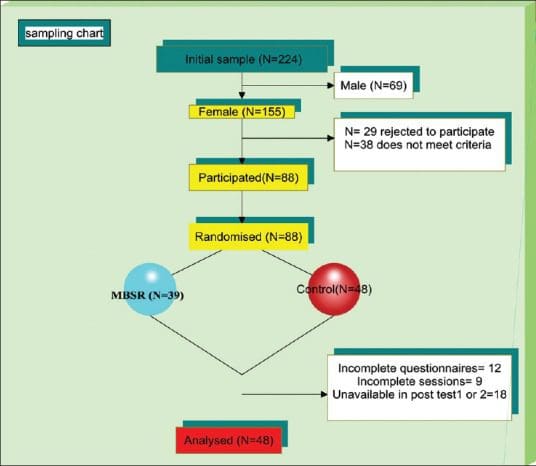
Out of initial female samples aged 30–45 (n = 155) who diagnosed as chronic NSLBP by physicians in physiotherapy centers of Ardebil-Iran at least 6 months before. Only 88 met inclusion criteria and gave consent to participate in the research program. Patients were randomly assigned in small groups to receive MBSR plus medical usual care (experimental group) and medical usual care (control group). Some patients dropped during and after the treatment. The final sample of the study comprised of 48 females.
Inclusion Criteria
- Age 30–45 years
- Being under medical treatments like physiotherapy and medicine
- Medical problem-history of NSCLBP and persisting pain for at least 6 months
- Language – Persian
- Gender – female
- Qualification – educated at least up to high school
- Consent and willingness to alternative and complementary therapies for pain management.
Exclusion Criteria
- History of spine surgery
- Combination with other chronic disease
- Psychotherapy in the last 2 years excluded
- Unavailability in next 3 months.
The proposal of study approved by the scientific committee of “Panjab University,” psychology department and all patients signed consent to participate in the present study. The study approved in India (in the university which researcher done her PhD), but conducted in Iran because researcher is from Iran originally and there was language and culture difference problem. Approval from Institutional Ethics Committee of physiotherapy center of Ardebil was obtained in Iran also to carry out the research.
Design
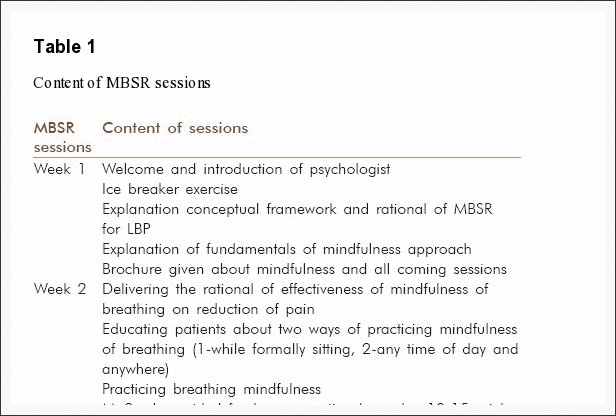
The study made use of the pre-post quasi time series experimental design to assess the efficacy of MBSR in 3 times frames (before-after-4 weeks after the program). A MBSR program administered one session per week for explaining techniques, practice, and feedback and share their experience for 8 weeks beside 30–45 min’ daily home practice [Table 1]. The intervention was conducted in three groups included 7–9 participants in each group. The process of framing the program was based on the quid lines provided by Kabat-Zinn, Morone (2008a, 2008b and 2007)[6,12,13,14] and some adaptation done for the patients involved in the study. The control group was not offered any type of intervention in the research project. Consequently, they underwent the normal routines in healthcare including physiotherapy and medicine.
Intervention
The sessions conducted in a private physiatrist clinic near to physiotherapy centers. Sessions took 8 weeks, and each session lasted for 90 min. Meditation transformed the patients’ awareness through the techniques of breathing and mindfulness. The intervention was conducted in small groups included 7–9 participants in each group. Table 1 for details of session’s content which prepared according books and previous studies.[6,12,13,14]
Assessments
The questionnaire completed by patients before the intervention, after intervention and 4 weeks after the interventions. The receptor of physiotherapy centers conducted the assessment. The receptors trained before conducting the assessment, and they were blind for the hypothesis of the study. The following are used for assessment of participants:
McGill Pain Questionnaire
The main component of this scale consists of 15 descriptive adjectives, 11 sensory including: Throbbing, Shooting, Stabbing, Sharp, Cramping, Gnawing, Hot-burning, Aching, Heavy, Tender, Splitting, and four affective including: Tiring-exhausting, Sickening, Fearful, Punishing-cruel, which are rated by the patients according to their severity on a four point scale (0 = none, 1 = mild, 2 = moderate, 3 = severe), yielding three scores. The sensory and affective scores are calculated by adding sensory and affective item values separately, and the total score is the sum of the two above-mentioned scores. In this study, we just used pain rating index with total scores. Adelmanesh et al.,[15] translated and validated Iran version of this questionnaire.
Quality of Life (SF-12)
The quality of life assessed by the validated SF-12 Health Survey.[16] It was developed as a shorter, quicker-to-complete alternative to the SF-36v2 Health Survey and measures the same eight health constructs. The constructs are: Physical functioning; role physical; bodily pain; general health; vitality; social functioning; role emotional; and mental health. Items have five response choices (for example: All of the time, most of the time, some of the time, a little of the time, none of the time), apart from two questions for which there are three response choices (for the physical functioning domain). Four items are reverse scored. Summed raw scores in the eight domains are transformed to convert the lowest possible score to zero and the highest possible score to 100. Higher scores represent better health and well-being. The standard form SF-12 uses a time frame of the past 4 weeks.[16]
The Iranian version of SF-12 in Montazeri et al. (2011) study showed satisfactory internal consistency for both summary measures, that are the Physical Component Summary (PCS) and the Mental Component Summary (MCS); Cronbach’s α for PCS-12 and MCS-12 was 0.73 and 0.72, respectively. The known – group comparison showed that the SF-12 discriminated well between men and women and those who differed in age and educational status (P < 0.001) 2.5.[17]
Statistical Analysis
The SPSS 20 (Armonk, NY: IBM Corp) was used to analysis of data. For descriptive analysis mean, standard deviation (SD) used. For performing ANCOVA, the pretest scores were used as covariates.
Results
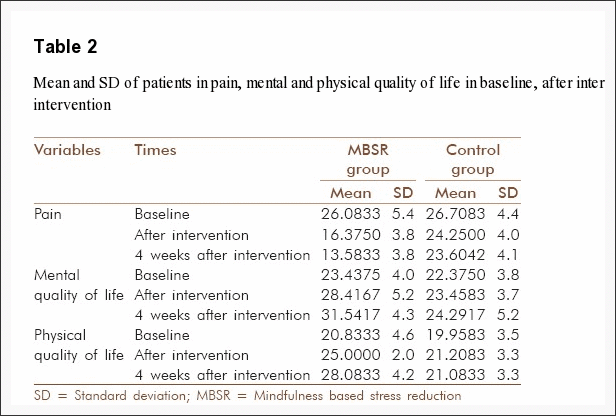
The mean age was 40.3, SD = 8.2. 45% of females were working and the rest were a house wife. 38% had two children, 55% one child and the rest did have children. All were married and from middle-income families. 9.8% of patients reported very low physical quality of life, and the rest were low (54.8%) and moderate (36.4%). This was 12.4%, 40% and 47.6% very low, low and medium levels of mental quality of life in patients participated in our study (n = 48). The mean and SD of patients in MBSR and control group showed a decrease in pain and increase in mental and physical quality of life [Table 2].
Comparative Results
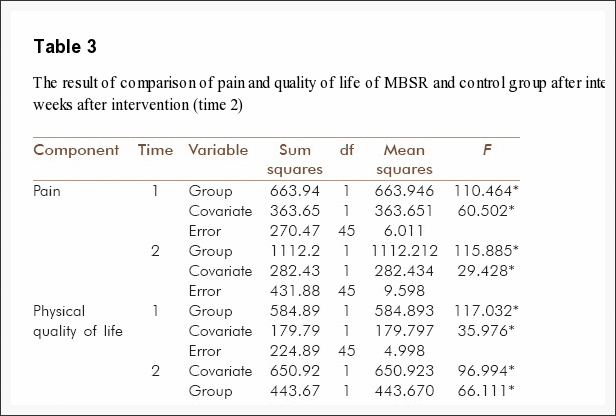
Pain. The results indicated that after adjusting for pretest scores, there was a significant effect of the between subject factor group (F [1, 45] =110.4, P < 0.001) and (F [1, 45] =115.8, P < 0.001). Adjusted post-test scores suggest that the intervention had an effect on increasing the pain scores of the NSCLBP patients who received the MBSR as compared to those who were in the control group and did not receive any mind-body therapy [Table 3].
Quality of life. The results shows that after adjusting for pretest scores, there was a significant effect of the between subject factor group (F [1, 45] =16.45, P < 0.001) and (F [1, 45] =21.51, P < 0.001). Adjusted post-test scores suggest that the intervention had an effect on increasing the physical quality of life scores of the NSCLBP patients who received the MBSR as compared to those who were in the control group and did not receive any mind-body therapy [Table 3].
The results also showed that after adjusting for pretest scores, there was a significant effect of the between subject factor group (F [1, 45] =13.80, P < 0.001) and (F [1, 45] =25.07, P < 0.001). Adjusted post-test scores suggest that the intervention had an effect on increasing the mental quality of life scores of the NSCLBP patients who received the MBSR as compared to those who were in the control group and did not receive any psychological therapy [Table 3].

Dr. Alex Jimenez’s Insight
Mindfulness is the psychological process which involves activating a brain relaxation pathway by intentionally ignoring mental “chatter”, bringing one’s attention to experiences occurring in the present moment and focusing on your breathing. Mindfulness can commonly be achieved through the practice of meditation and stress management methods and techniques. According to research studies, mindfulness is an effective treatment option which can help decrease chronic low back pain. Researchers have previously compared mindfulness-based stress reduction, or MBSR, with cognitive behavioral therapy to determine whether these mindfulness interventions could improve chronic low back pain. The following article was also conducted to determine if mindfulness meditation is an effective treatment option for chronic low back pain. The results of both research studies were promising, demonstrating that mindfulness can be more effective for chronic low back pain than traditional treatment options as well as the use of drugs and/or medication.
Discussion
The results showed that the experimental group who were subjected to the MBSR showed a significant improvement in their overall pain severity, physical and mental quality of life scores due to the training received as compared to the control group who received only usual medical care. The program reduced pain perception and enhanced both physical and mental quality of life and impacted on the experimental group clearly in comparison of the usual medical care. Baranoff et al., 2013,[18] Nyklícek and Kuijpers, 2008,[19] and Morone (2) et al., 2008[20] reported the same results.
Kabat-Zinn et al. believed the process of pain reduction occurred by “uncoupling” the physical sensation, from the emotional and cognitive experience of pain, the patient is able to reduce the pain.[21] In the current study, the participants uncoupled the different components of the experience of pain. Breathing exercise distract their mind from pain to breathing and mindful living made them aware about maladaptive coping strategies.
In the first session, information given about the fundamentals of mindfulness, describing the mindfulness supporting attitudes included being nonjudgmental toward thought, emotions or sensations as they arise, patience, nonstriving, compassion, acceptance and curiosity gave them a wisdom and believe that they are suffering from painful thoughts more than the pain itself.
Furthermore, during body scan practice they learned to see their real body conditions, as it truly was, without trying to change the reality. Accepting their chronic illness condition helped them see the other possible abilities in their social and emotional roles. In fact the body scan practice helped them change the relationship with their body and pain. Through direct experience in body scan, one realizes the interconnection between the state of the mind and the body, and thereby increases patients’ self-control over their life. Mindful living techniques also improved their quality of life by teaching them to pay more attention to their daily life necessities, which led to the experience of subtle positive emotions, like peace and joy, self-esteem and confidence. Furthermore, they appreciated positive things. Once they learned to see the persistent pain objectively and observe other sensations in their body, they applied the same principles through mindful living techniques in their everyday life. As a result, they learned how to manage their health and began to engage in their duties mindfully.
A number of research studies such as Plews-Ogan et al.,[22] Grossman et al.,[23] and Sephton et al., (2007)[24] showed effectiveness of mindfulness meditation program on quality of life of patients with chronic pain conditions.
Conclusion
All together the result of this study and previous studies highlighted the effectiveness of complementary and alternative treatment for patients with chronic LBP. Regarding the considerable role of quality of life in professional and personal life designing the effective psychotherapies especially for enhancement of quality of life of patients with chronic LBP strongly suggested by the authors.
This study involved with several limitations such as ununiformed usual care received by patients. The provided physiotherapy sessions or methods and medicine prescribed by different physicians in slightly different manner. Although some patients commonly dose not completed physiotherapy sessions. The sample size was small and it was only limited to three centers. This is suggested for future researchers to conduct study with considering physiologic variables such as MRI, NMR and neurologic signals to test the efficacy of MBSR to decrease pain sufferer.
In conclusion, more evidence-based larger scale researches with longer-term follow-up need to be done to increase the therapeutic weight and value of MBSR as a part of complementary alternative medicine being preventive and rehabilitation method among CLBP patients.
Acknowledgement
We are thankful from patients who were corporate with us. Dr. Afzalifard and staff of physiotherapy centers of Ardebil.
Footnotes
- Source of support: Nil.
- Conflict of interest: None declared.
In conclusion, mindfulness is the most prevalent treatment with the best supporting evidence towards improving and managing chronic low back pain. Mindfulness interventions, such as mindfulness-based stress reduction and cognitive behavioral therapy, have demonstrated to be effective for chronic low back pain. Furthermore, mindfulness meditation was also demonstrated to effectively help improve as well as manage chronic low back pain caused by stress. However, further research studies are still required to determine a solid outcome measure for mindfulness interventions and chronic pain. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez

Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.

EXTRA IMPORTANT TOPIC: Managing Workplace Stress
MORE IMPORTANT TOPICS: EXTRA EXTRA: Choosing Chiropractic? | Familia Dominguez | Patients | El Paso, TX Chiropractor
[/et_pb_text][et_pb_accordion _builder_version=”3.0.106″][et_pb_accordion_item _builder_version=”3.0.106″ title=”Blank” use_background_color_gradient=”off” background_color_gradient_start=”#2b87da” background_color_gradient_end=”#29c4a9″ background_color_gradient_type=”linear” background_color_gradient_direction=”180deg” background_color_gradient_direction_radial=”center” background_color_gradient_start_position=”0%” background_color_gradient_end_position=”100%” background_color_gradient_overlays_image=”off” parallax=”off” parallax_method=”on” background_size=”cover” background_position=”center” background_repeat=”no-repeat” background_blend=”normal” allow_player_pause=”off” background_video_pause_outside_viewport=”on” text_shadow_style=”none” box_shadow_style=”none” custom_css_main_element=”display:none;” /][et_pb_accordion_item _builder_version=”3.0.106″ title=”References” use_background_color_gradient=”off” background_color_gradient_start=”#2b87da” background_color_gradient_end=”#29c4a9″ background_color_gradient_type=”linear” background_color_gradient_direction=”180deg” background_color_gradient_direction_radial=”center” background_color_gradient_start_position=”0%” background_color_gradient_end_position=”100%” background_color_gradient_overlays_image=”off” parallax=”off” parallax_method=”on” background_size=”cover” background_position=”center” background_repeat=”no-repeat” background_blend=”normal” allow_player_pause=”off” background_video_pause_outside_viewport=”on” text_shadow_style=”none” box_shadow_style=”none”]
[/et_pb_accordion_item][et_pb_accordion_item _builder_version=”3.0.106″ title=”Close Accordion” use_background_color_gradient=”off” background_color_gradient_start=”#2b87da” background_color_gradient_end=”#29c4a9″ background_color_gradient_type=”linear” background_color_gradient_direction=”180deg” background_color_gradient_direction_radial=”center” background_color_gradient_start_position=”0%” background_color_gradient_end_position=”100%” background_color_gradient_overlays_image=”off” parallax=”off” parallax_method=”on” background_size=”cover” background_position=”center” background_repeat=”no-repeat” background_blend=”normal” allow_player_pause=”off” background_video_pause_outside_viewport=”on” open_toggle_background_color=”#ffffff” closed_toggle_background_color=”#ffffff” text_shadow_style=”none” custom_padding=”0px|||” custom_padding_tablet=”0px|||” custom_padding_phone=”0px|||” box_shadow_style=”none” custom_css_main_element=”border:none;” custom_css_toggle_title=”font-size:0.8em;” custom_css_toggle_icon=”display:none;” /][/et_pb_accordion][/et_pb_column][/et_pb_row][/et_pb_section]
Post Disclaimer
Professional Scope of Practice *
The information herein on "Effectiveness of Mindfulness on Herniated Discs & Sciatica in El Paso, TX" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Our information scope is limited to Chiropractic, musculoskeletal, physical medicines, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somatovisceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and/or functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and directly or indirectly support our clinical scope of practice.*
Our office has reasonably attempted to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez, DC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, RN*, CCST, IFMCP*, CIFM*, ATN*
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807, New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Florida
Florida License RN License # RN9617241 (Control No. 3558029)
License Compact Status: Multi-State License: Authorized to Practice in 40 States*
Presently Matriculated: ICHS: MSN* FNP (Family Nurse Practitioner Program)
Dr. Alex Jimenez DC, MSACP, RN* CIFM*, IFMCP*, ATN*, CCST
My Digital Business Card