


Table of Contents
Pyogenic Spinal Infection
- aka Spondylodiscitis and vertebral osteomyelitis overall are relatively infrequent and may present with bimodal distribution: children and adults >50’s
- Occasionally considered as two separate entities due to variations in
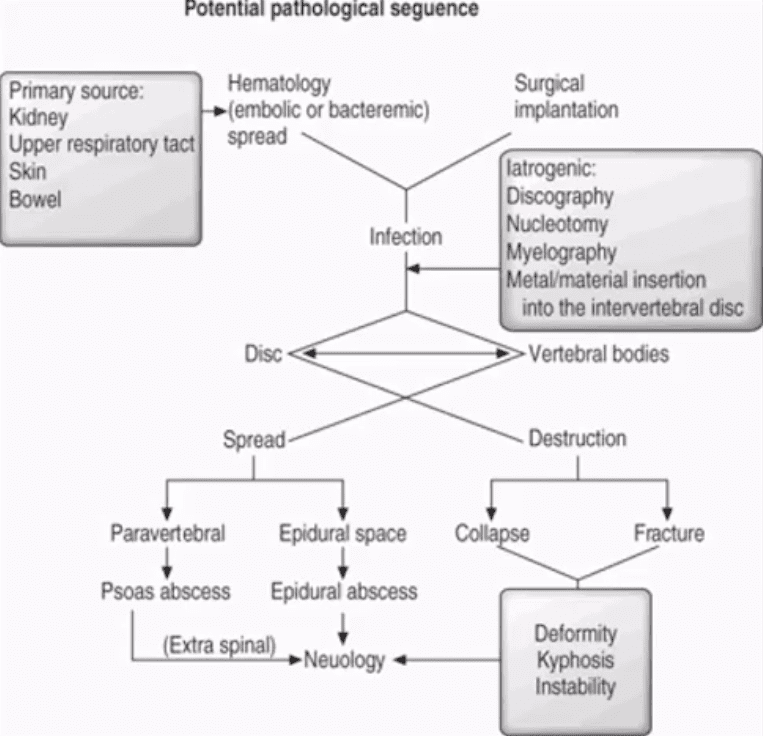
blood supply of pediatric vs. adult spines - Risk factors/causes: distant site of infection in the body (25-35%) e.g. oropharynx, urogenital infections, bacterial endocarditis, indwelling catheters, florid skin infections furunculosis/abscess etc.
- Iatrogenic: operative (e.g. discectomy) interventional or diagnostic/therapeutic procedures
- Penetrating trauma
- Immunocompromised patients
- Diabetics
- Malnourished patients or patients with low protein
- IV drug users
- Chronic
diseas patients,cnacer patients etc.
Potential Pathological Sequence
Clinical Presentation
- Back pain with or w/o high fever and other “septic” signs. Fever may only present in 50
% children - Exacerbation of pre-existing back pain in post-surgical cases
- Neurological complications in advanced cases of vertebral destruction and epidural abscess
- Meningitis, septicemia etc.
- Labs: Blood tests are unspecific, may or may not indicate elevated ESR/CRP, WBC
- Diagnostic imaging is important but
- If clinical suspicion is strong, prompt I.V. antibiotics are needed to prevent serious complications
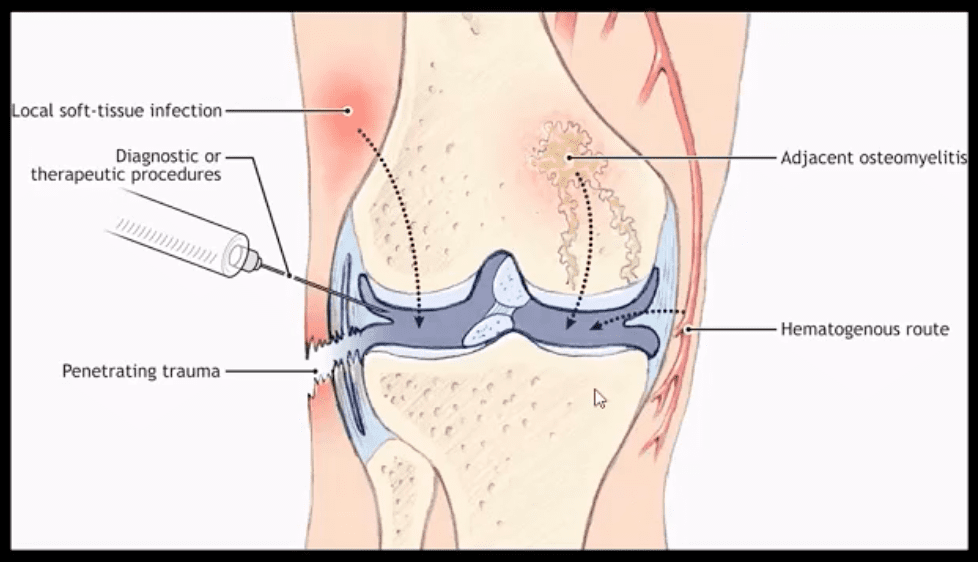
Routes of Infection
- Infection routes to the spine
are similar to bone in general - 3-distinct routes:
- 1) Hematogenous spread as bacteremia (most common)
- 2)
Adjacent site of infection (e.g. soft tissue abscess) - 3)Direct inoculation (e.g. iatrogenic or traumatic)
- M/C organism Staph. Aureus
- Mycobacterium TB (tuberculous spinal osteomyelitis) aka Pott’s disease can be presented in cases of re-activated or disseminated pulmonary TB
Mechanisms of Spinal Infection
- May vary depending on the patients’ age
- In children, the IVD receives direct blood supply and can be infected directly spreading to adjacent bone and causing spondylodiscitis
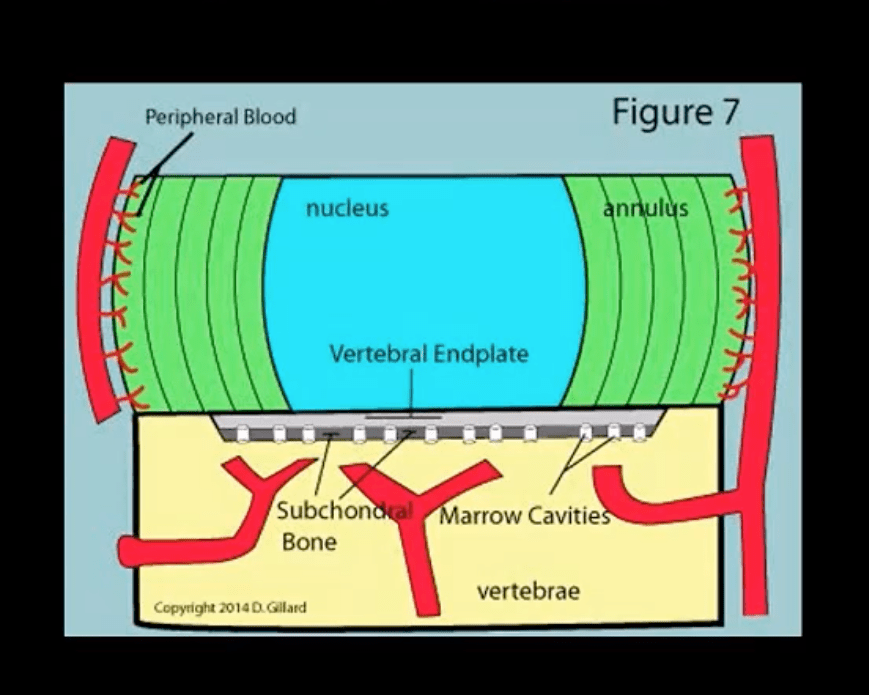
In Adults
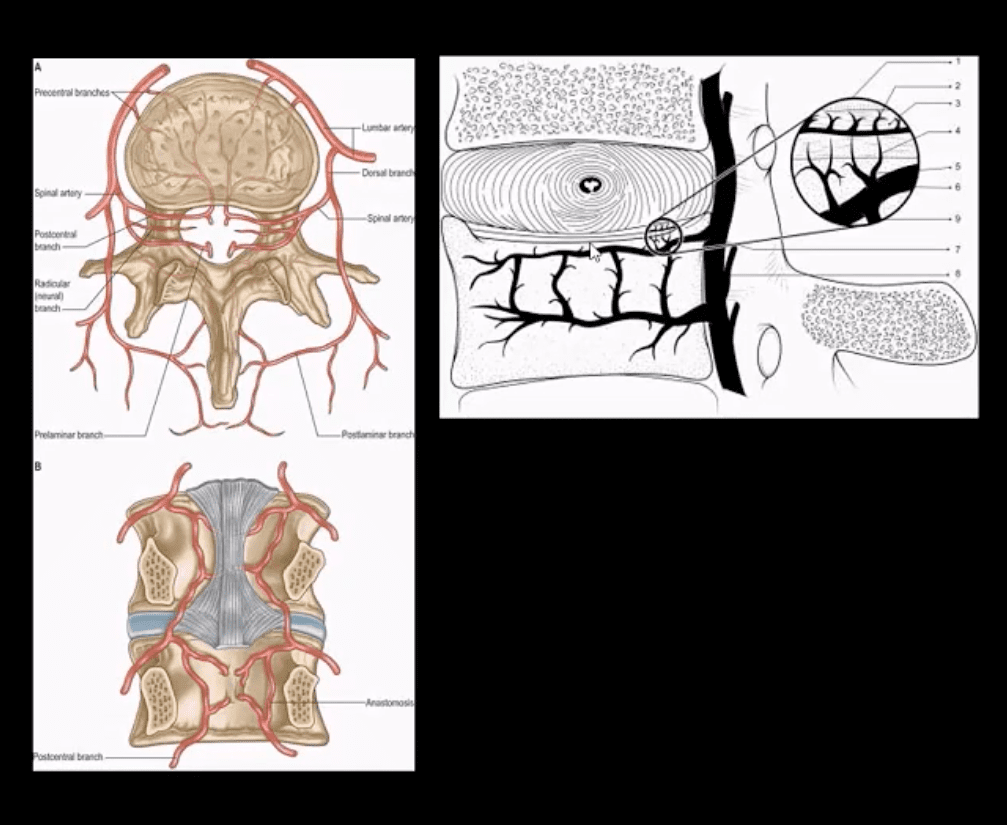
- The disc is avascular
- Pathogens invade adjacent vertebral end-plates via end-arterial supply of the vertebral body that mayfacilitate infectiondue to slow turbulent flow
- Organisms may then quickly gain access to disc substance rich in nutrients (discitis) often w/o mojor initial visible destruction to the bone
- Thus, one of the earliest rad. findings of spinal infection is sudden reduction of disc height
- Later end-plate irregularity/sclerosis may develop, subsequently affecting the entire adjacent vertebral bodies
Diagnostic Imaging
- Initially in most cases of MSK complaints, radiography is the 1st imaging step
- Initially X-radiography is often unrewarding and may appear unremarkable for 7-10 days or presents with some subtle soft tissue changes (e.g. obscuration of Psoas shadows etc.)
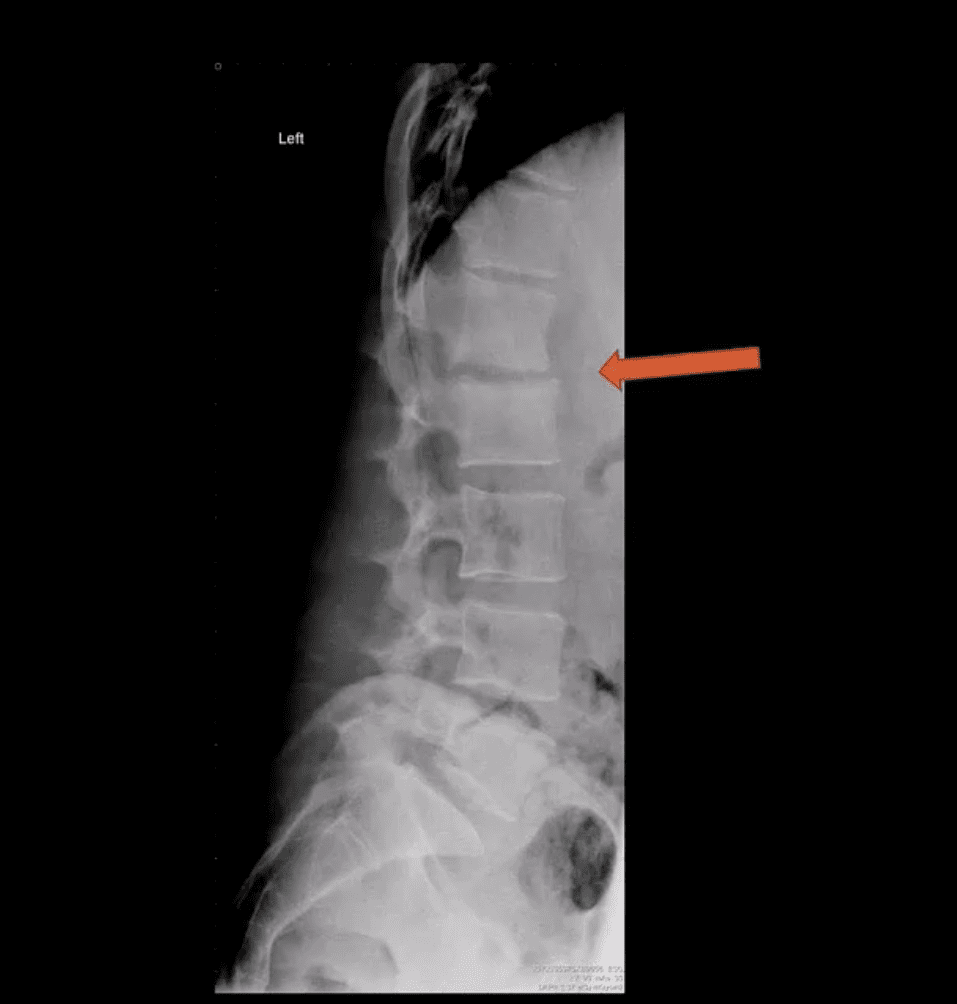
- Someof the earliest x-ray signs of pyogenic spondylodiscitis: sudden reduction of disc height (above arrow) during initial 7-10 days
- Subsequently (10-20 days) some end-plate irregularity and adjacent sclerosis may be noted
- In more advanced cases, subsequent vertebral destruction and collapse may occur
- N.B. Reliable feature to DDx between spinal infection and metastasis is the preservation of disc height in thelatter
Discitis
- Discitis needs to be DDx from DDD (spondylosis)
- An important DDx between discitis and DDD is lack of osteophytes (spondylophytes) and intradiscal gas (vacuum phenomenon) in DDD.
- In fact,
presence of intradiscal gas (vacuum phenomenon) virtually excludes discitis (except if gas-forming pathogens are involved) - Note: sudden disc narrowing with no appreciable spondylosis (above
first image) is suspicious for infection (discitis) - MRI +C is required to evaluate suspected infection
- N.B. 50-60% of pyogenic spondylodiscitis occur in the lumbar region
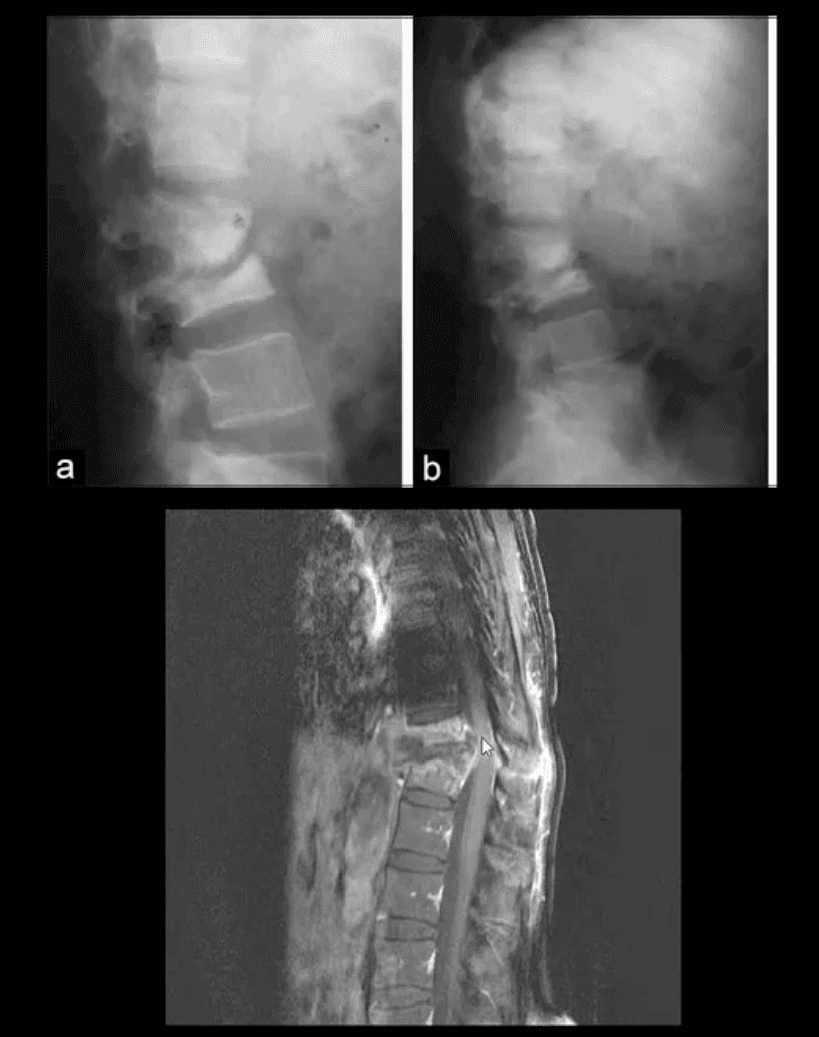
AP & Lateral Lumbar Radiographs
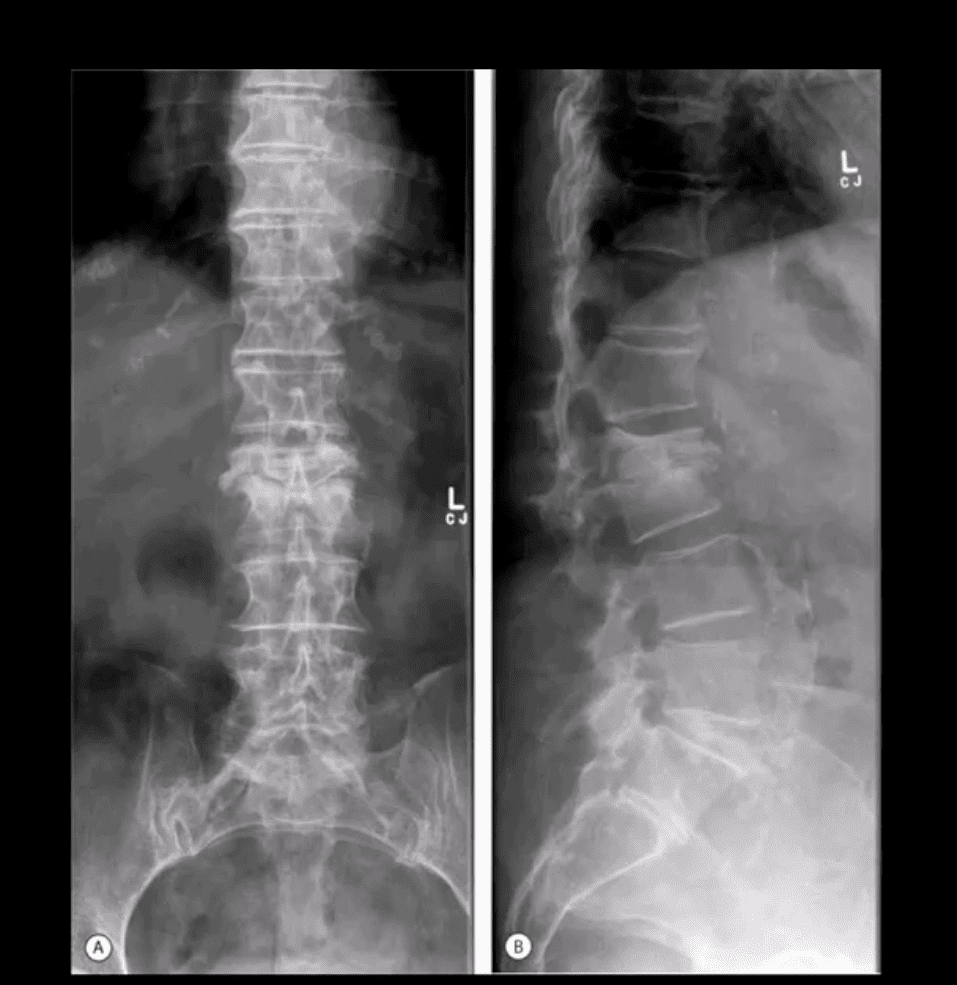
- Note severe disc narrowing and adjacent vertebral body destruction at L1-L2 in a 68 -y.o.-female with a known Hx of type 2 DM
- Additional imaging modalities should be used to support the Dx
- Final Dx: Pyogenic Spondylodiscitis
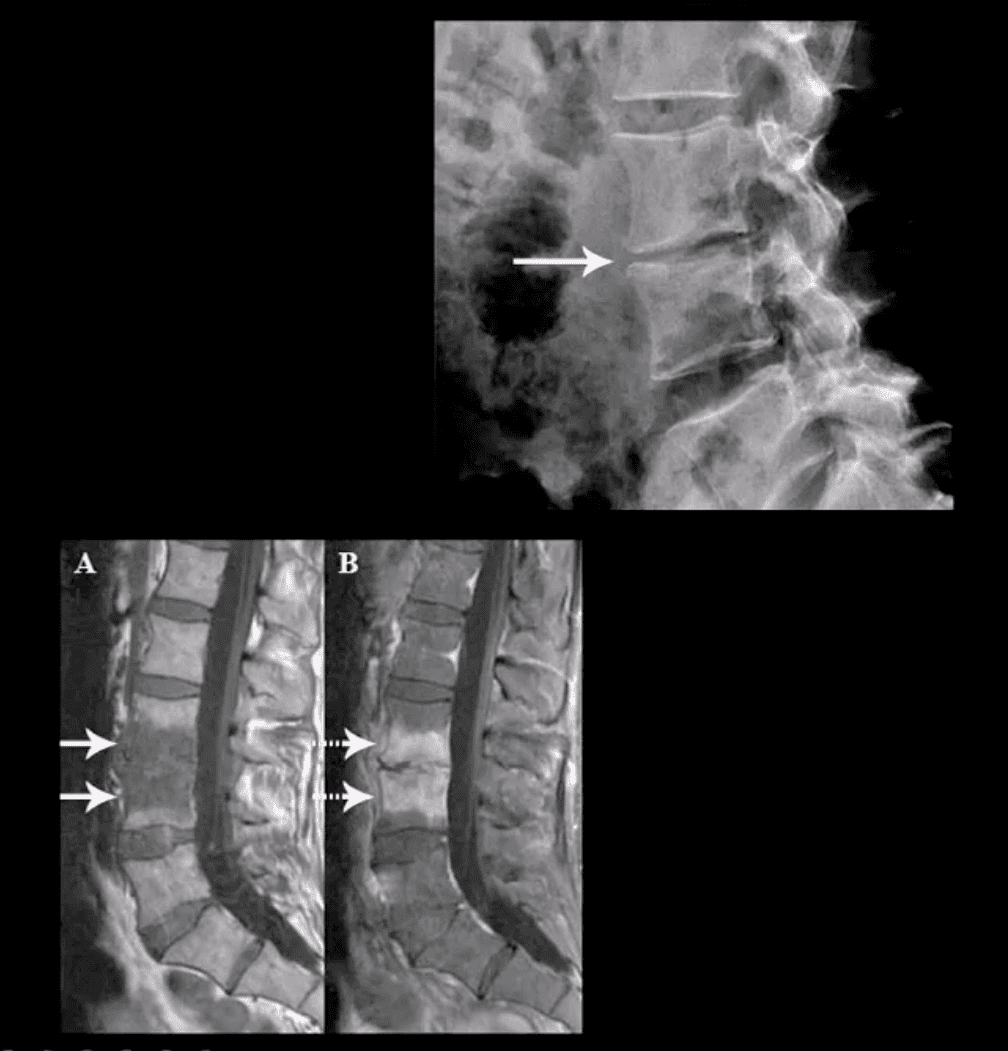
Sagittal T1 & T2 MRI

- Weighted MRI slices of a patient who had laminectomy at L4
- MR imaging with gad contrast is the modality of choice for Dx of spinal infection
- Early septic changes affecting the disc and adjacent vertebral end-plates are readily demonstrated as a low signal on T1 and high T2/STIR d/t edema and inflammation
- T1 FS +C gad images show avid enhancement of the lesion due to granulation tissue around the phlegmon. Peripheral enhancement is also characteristic of an abscess.
- Epidural extension/abscess can also be successfully detected my MRI
- N.B. 50% of epidural abscess cases present with neurological signs
STIR & T1 FS +C Gad Sagittal MRI

- Marked septic collection and edema affecting L4-5 disc and vertebral body with some epidural extension and paraspinal soft tissue edema. Avid contrast enhancement is noted surrounding low signal foci within the bone and disc tissue, some gad. Enhancement is noted in posterior paraspinal muscles and dural spaces
- Management: Dx of spondylodiscitis requires prompt I.V antibiotics. If instability and neurological complications develop referral to a Neurosurgeon is required
MRI Unavailable or Contraindicated
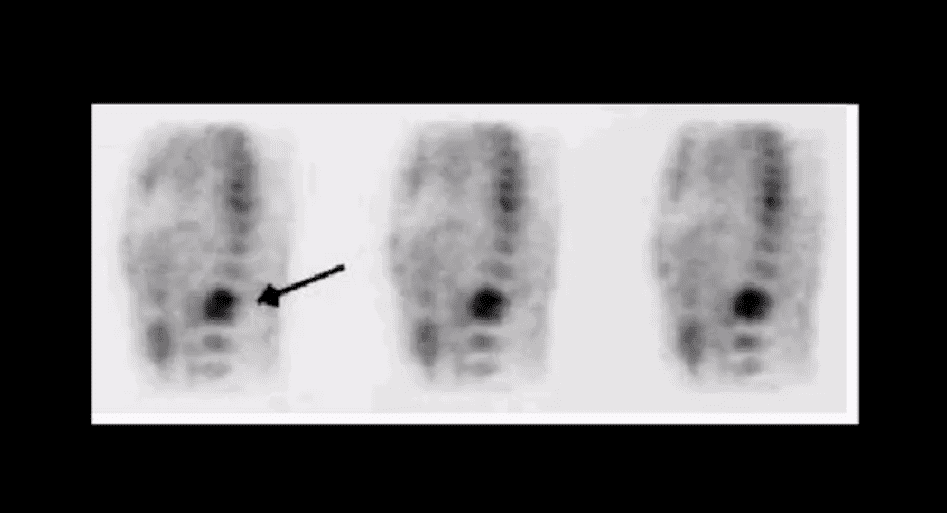
- Bone scintigraphy is very sensitive but non-specific for spinal infection but overall is of great value d/t higher sensitivity than x-rays and relatively low cost.
- An area of increased flow with radiopharmaceutical uptake is characteristic but not specific sign of spondylodiscits
- If neurological signs are present and MRI is contraindicated than CT myelography may be used
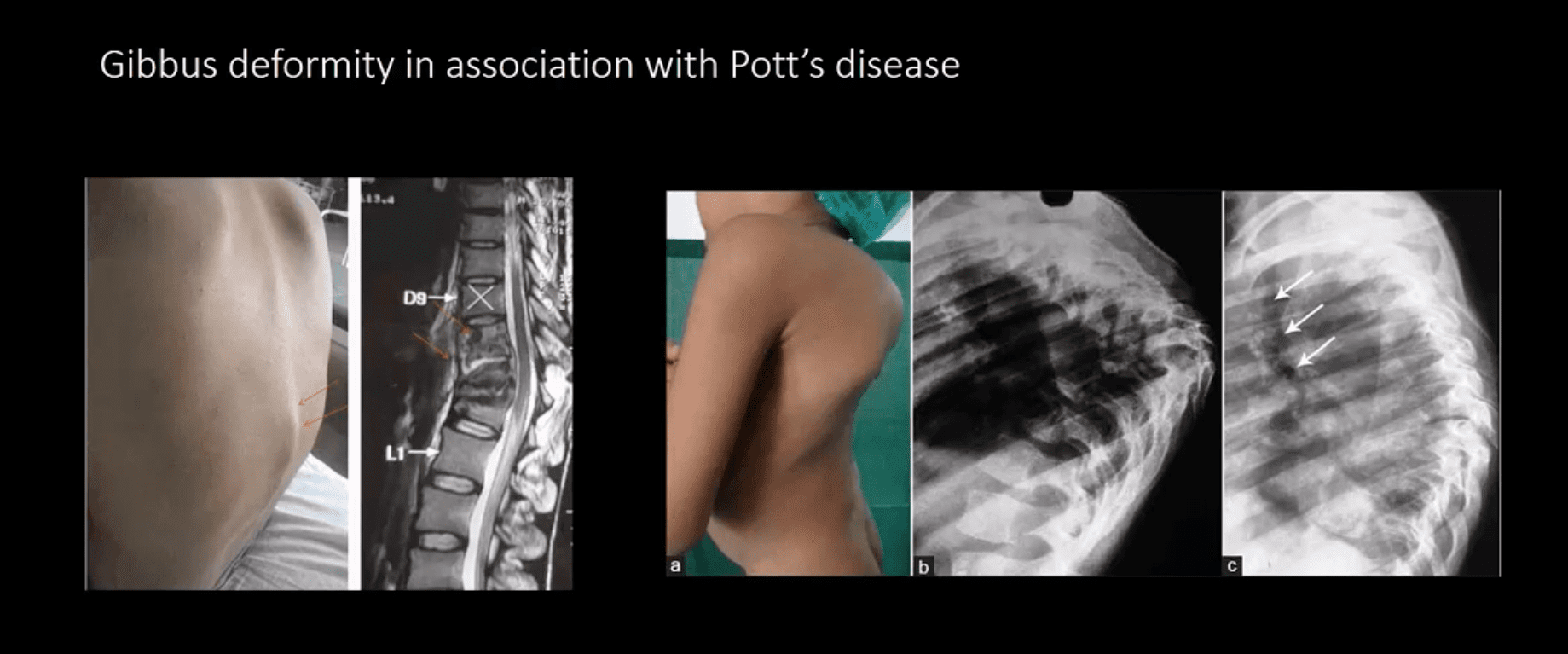
TB Osteomyelitis aka Pott’s Disease
- TB osteomyelitis is increasing d/t HIV and other immunocompromised states. Extrapulmonary TB m/c affects the spine and especially the thoracic spine (60%)
- Radiographic Pathology: TB bacillus infects vertebral body and often spreads
subligamentously . “Cold” paraspinal abscess collection may develop and spreads along fascial planes e.g. Psoas abscess. Disc spaces are preserved until v. late and skip areas are noted helping to DDx TB from pyogenic infection. Severe vertebral destruction aka Gibbus deformity may develop (>60-degree sometimes) and may become permanent. Neurologic and many regional complications may develop - Imaging approach: CXR with
spinal x-rays 1st step that may be unrewarding but may potentially reveal VB destruction w/o disc narrowing. CT scanning is more superior than x-rays. MRI with gad C is a modality of choice - Management: isoniazid, rifampin, operative.
- DDx: Fungal/Brucella infection, neoplasms, Charcot spine
Gibbus Deformity & Pott’s Disease
Infection Of The Spine
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Comments are closed.