

Among the general population of athletes, stress fractures can be a rare cause of pain, accounting for only 2 percent of all reported sports injuries. However, a considerably higher number of stress fractures are diagnosed in long distance runners and triathletes.
Stress fractures occurring around the pelvis are significantly uncommon although, a majority of them are often considered a differential diagnosis when athletes, specifically long distance runners and triathletes, report hip, groin or buttock pain during and after running. Because stress fractures around the pelvic/hip region, including the sacral, pubic rami and femoral neck region, are rarely diagnosed, understanding and discussing the anatomy of the injury, their clinical presentation, diagnosis and treatment for each of these types of stress fractures is important for an athlete in order to find a solution for those who do encounter it.
Table of Contents
How Stress Fractures Occur
Stress fractures occur over a determined period of time when the bone is no longer capable of withstanding submaximal, repetitive forces. They frequently result when normal stresses cause bone fracture with decreased bone density, such as in an elderly osteoporotic individual, or as a result of an abnormal stress being placed against a normal bone and causing a fracture, such as in a long distance runner.
When the bones are exposed to loading, the introductory physiological response is a respective increase in osteoclastic activity, or bone resorption, leading to temporary structural weakening before new bone formation. If these stresses continue to occur without having the bone properly adjust to this additional, ongoing osteoclastic activity, the pressure may exceed bone regeneration, causing microfractures to occur.
The first characteristic of a stress reaction observed through the use of MRI is bone oedema as well as increased activity on bone scan. Bone scan in the acute phase has high sensitivity but an increased uptake may also be due to infection, bone infarction or neoplastic activity. Researchers from previous studies stated that 60 to 70 percent of X-rays in the acute phase of stress fractures, approximately less than 2 weeks after the injury, have a negative result. Due to its high sensitivity as well as a lack of radiation and high specificity, even despite its elevated cost, MRI is often the preferred procedure to identify stress fractures in their early phases.
Various distinct intrinsic and extrinsic elements have been determined as risk factors for stress fractures. These include but are not limited to: biomechanics, strength and flexibility, nutrition, hormonal and menstrual disturbances, and footwear. These must all be considered prior to assessing an individual with a suspected stress fracture. During an analysis of 8 female athletes with sacral stress fractures, the most significant risk factor for these types of fractures was the rapid increase in impact activity during more intense exercise programs. An increase in workload should thus be considered a significant risk factor for stress fractures.
Anatomy of Sacral Stress Fractures
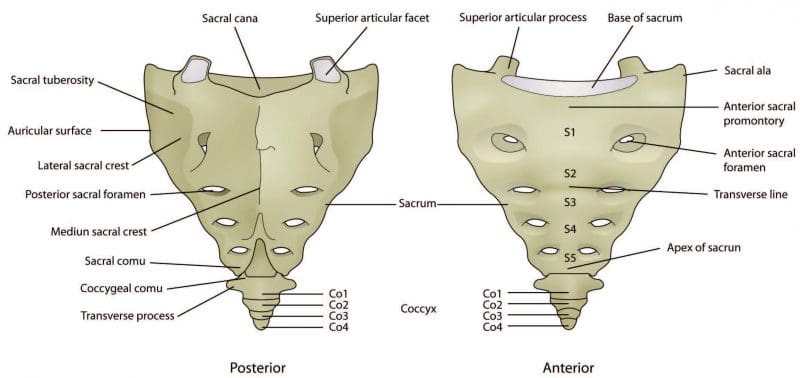
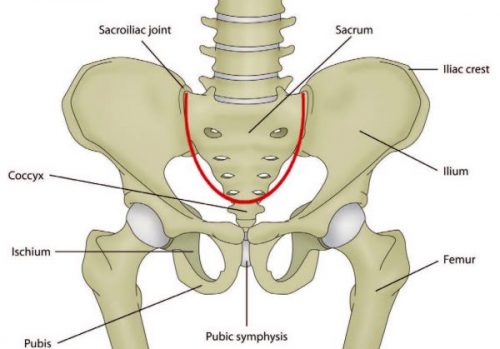
The sacrum consists of 5 fused vertebrae, S1 to S5, and is triangular in shape. It connects with the ilium at the sacroiliac joint and, due to its shape and function to distribute forces, it’s often described as the foundation to the arch of the pelvis. The sacrum, much like an inverted arch, supports the entire weight of the upper body and transfers force to the pelvis.
Sacral stress fractures most commonly occur in the lateral portion of the sacrum and are more frequently diagnosed in women. It’s been hypothesized that the shape of the female pelvis can lead create difficulty when distributing weight through the sacrum than the average male pelvis. However, it’s also been reported that several male elite Australian triathletes have experienced sacral stress fractures in recent years.
Symptoms
An athlete with a sacral stress fracture will often manifest acute onset back, buttock or hip pain which is generally described to occur suddenly during a run, making them incapable of continuing at the time. The individual may also experience limited mobility and they could or could not suffer pain on the palpation of the sacrum. Additionally, they may not experience any neurological symptoms but symptoms of sciatica may be common during this type of stress fracture. Sciatica can include pain, weakness or numbness and burning or tingling sensations along the lower back, buttock or hip, often radiating down the thigh. The individual may suffer pain or tightness when walking and they will experience symptoms when hopping on the affected side. Athletes with sacral stress fractures also frequently report pain during single leg loading tasks, for example, when putting pants on.
Diagnosis
Due to the extreme overlying soft tissue and complex bone anatomy, simple radiographs can rarely conclude the presence of a sacral stress fracture. Bone scan, MRI or CT can be utilized to effectively diagnose a sacral stress fracture. CT and MRI findings suggest that sacral stress fractures occur as a result of constant compressive forces which lead to microfractures of the trabecular bone. These fractures infrequently develop a visible callus on plain radiograph, therefore, MRI or CT scans should be utilized as a follow up imaging if poor healing is detected.

Treatment
The progression of treatment for an athlete with a sacral stress fracture broadly depends on the athlete’s symptoms as these are generally stable fractures. Rehabilitation procedures will progress from non-weight bearing to weight bearing to progressive return to running activities as the symptoms decrease. In most cases, a period of 6 weeks with no running followed by a 6 to 8-week period of a return to running progression may be required. A majority of published works indicate athletes may have a full return to activity by 4 months with rare cases taking up to 14 months.
Repeated CT scans approximately 4 and 8 months after the individual’s original diagnosis can often display no signs of previous fractures which demonstrate a quicker and fuller healing of the well-vascularized trabeculae microfractures when compared to fractures involving the less well-vascularized cancellous bone. Researchers concluded that women with sacral stress fractures who had the best diets and fewer prior stress injuries or menstrual irregularities, healed the fastest.
Anatomy of Pubic Rami Stress Fractures
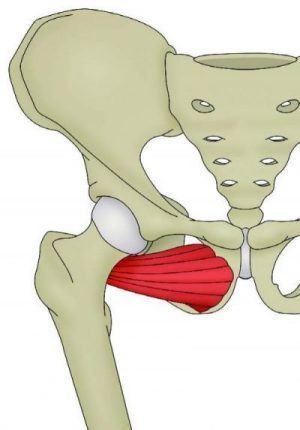
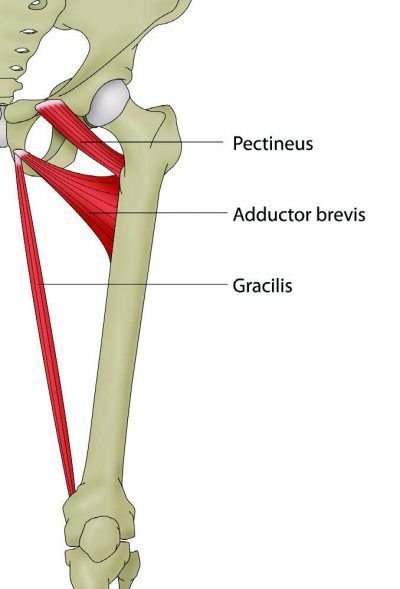
The inferior pubic ramus slopes downward and medial from the superior ramus, narrowing as it goes down and it is the region where the adductor magnus, brevis and gracilis connect, including the obturator internus and externus. Pubic Rami stress fractures have been diagnosed among runners, triathletes and military service members. These generally occur in the inferior pubic rami next to the pubic symphysis. Researchers proposed that these fractures are a result of repetitive forces being applied to and transmitted to the bone through muscle contraction or fatigue. In a study on female military service members, it was suggested that over-striding during marching procedures was a potential factor contributing to pubic rami stress fractures.
Symptoms
Pubic rami stress fractures are generally detected either in competitive races or during intensive training sessions. These frequently occur at the insertion of the adductors and/or external rotators of the hip. Athletes with pubic rami stress fractures commonly suffer from pain in the hip, buttock, inguinal or adductor region which increases with activity and decreases with rest. It’s important to remember that pain caused by irritation and swelling along these regions may also cause symptoms similar to sciatica. It’s important to receive a proper diagnosis to rule out a compression of the sciatic nerve which could be causing neurological symptoms. Athletes with this type of injury often limp and on clinical testing, they may experience symptoms with passive hip abduction, resisted hip adduction and resisted hip external rotation. Stress fractures of the pelvis can be determined even without radiographic evidence if the following criteria are met by an individual. First, running will be impossible for the athlete as a result of severe discomfort in the groin area. Then, the individual will experience discomfort in the groin with an unsupported stance on the affected leg. And last, an athlete may suffer symptoms of pain and tenderness after deep palpation procedures.
Diagnosis
Simple radiographs may demonstrate displaced fracture lines but a lack of radiographic evidence in the early phases of injury is not uncommon. Bone scan, CT or MRI may be used to determine the presence of fracture and bone oedema may be evident on MRI.
Treatment
These fractures tend to have a high rate for healing following 6 to 10 weeks of rest, however, they have a small risk of non-union and re-fracture if the appropriate amount of rest is not followed. Fractures that display delayed union will likely demonstrate full recovery when further conservative procedures are followed. Progression of treatment should be guided by pain and at first, the individual may require the utilization of crutches as walking may be painful.
Anatomy of Femoral Neck Stress Fractures
The femoral neck is the flattened, pyramid shaped piece of bone which connects the femoral head to the femoral shaft.
Athletes with femoral neck stress fractures generally report hip or groin pain when running. This pain usually has an insidious onset and the symptoms may become significantly worse depending on the intensity or duration of a run. At first, symptoms may occur at the end of a run but as the stress reaction worsens, the pain may begin showing earlier in the run where gradually more time may be required to relieve the pain and discomfort. Athletes with femoral neck stress fractures may experience hip and/or groin pain while resting and may suffer restless nights of sleep due to the symptoms. Often, individuals will also report pain while rolling in bed, single leg stance and during active straight leg raise.
Femoral neck stress fractures are described as either tension or compression stress fractures. Fracture displacement determines the outcome of an injury and tension stress fractures generally have a higher rate of displacement as a result of non-union, malunion or osteonecrosis. Due to this fact, tension stress fractures are considered more serious than compression fractures and may require surgical fixation.
Diagnosis
Conventional radiographs are often negative in the acute setting but may shown signs during instances where symptoms have been present for 2 weeks or more. MRI is the favored standard for diagnosis and should be ordered when a stress fracture of the femoral neck is suspected.
Treatment
Tension side stress fractures require diagnosis from a healthcare professional immediately after its occurred due to their risk of displacement. Compression side fractures are often managed conservatively with protected weight bearing and ongoing monitoring to keep track of the individual’s healing process. Initial phases of management should include non-weight bearing on crutches until there are no symptoms at rest, then progress to partial weight bearing to full weight bearing over a period of 4-6 weeks. A gradual return to run program can be started at 8 to 12-weeks of treatment, once the individual is able to properly walk without experiencing pain and other symptoms.
Return to Activity Plan
With all stress fractures located around the pelvis, a careful, gradual return to activity plan can be an essential element of the rehabilitation process. To make sure the athlete receives progressive loading without sudden increases in workload, the return to activity plan should be at least as long as the time off the individual’s specific activity. For instance, if the athlete had a sacral stress fracture which required 6 weeks of no running, then that athlete needs at least a 6-week gradual return to running plan before they can return to their previous running load.
Hip Strengthening Exercises
.video-container{position: relative; padding-bottom: 63%; padding-top: 35px; height: 0; overflow: hidden;}.video-container iframe{position: absolute; top:0; left: 0; width: 100%; height: 100%; border: none; max-width:100%!important;}
A strengthening program of the lower extremities can additionally be implemented early in the rehabilitation process, first beginning with non-weight bearing exercises, which can gradually change as the individual becomes able to weight bear without pain. Early strengthening can also help decrease muscle loss and address any biomechanical complications the athlete might be facing. As the stress fractures heal and the tolerance for load improves, these exercises can be progressed to other higher-load exercises to provide the athlete’s body for the return of their specific sports activity. 
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Sourced through Scoop.it from: www.elpasochiropractorblog.com
By Dr. Alex Jimenez

TRENDING TOPIC: EXTRA EXTRA: New PUSH 24/7®️ Fitness Center
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Comments are closed.