

Many types of arthritis can affect the structure and function of the muscles, bones and/or joints, causing symptoms such as, pain, stiffness and swelling. While arthritis can commonly affect the hands, wrists, elbows, hips, knees and feet, it can also affect the facet joints found along the length of the spine. One of the most well-known types of arthritis, known as rheumatoid arthritis or RA, is a chronic inflammatory disease of the joints which occurs when the human body’s own immune system attacks the synovium, the thin membrane that lines the joints. According to the article below, imaging the spine in arthritis is fundamental towards its proper treatment.
Table of Contents
Abstract
Spinal involvement is frequent in rheumatoid arthritis (RA) and seronegative spondyloarthritides (SpA), and its diagnosis is important. Thus, MRI and CT are increasingly used, although radiography is the recommended initial examination. The purpose of this review is to present the typical radiographic features of spinal changes in RA and SpA in addition to the advantages of MRI and CT, respectively. RA changes are usually located in the cervical spine and can result in serious joint instability. Subluxation is diagnosed by radiography, but supplementary MRI and/or CT is always indicated to visualize the spinal cord and canal in patients with vertical subluxation, neck pain and/or neurological symptoms. SpA may involve all parts of the spine. Ankylosing spondylitis is the most frequent form of SpA and has rather characteristic radiographic features. In early stages, it is characterized by vertebral squaring and condensation of vertebral corners, in later stages by slim ossifications between vertebral bodies, vertebral fusion, arthritis/ankylosis of apophyseal joints and ligamentous ossification causing spinal stiffness. The imaging features of the other forms of SpA can vary, but voluminous paravertebral ossifications often occur in psoriatic SpA. MRI can detect signs of active inflammation as well as chronic structural changes; CT is valuable for detecting a fracture.
Keywords: Spine, Arthritis, Rheumatoid Arthritis, Spondyloarthropathies
Introduction
The spine can be involved in most inflammatory disorders encompassing rheumatoid arthritis (RA), seronegative spondyloarthritides (SpA), juvenile arthritides and less frequent disorders such as, arthro-osteitis and SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome.
During the last decade, the diagnostic use of magnetic resonance imaging (MRI) and computed tomography (CT) has increased considerably, although radiography is still the recommended initial examination. It is therefore important to know the characteristic radiographic findings in arthritides in addition to the advantages of supplementary MRI and CT. This review will focus on the different imaging features and be concentrated on the most frequent inflammatory spinal changes seen in RA and SpA, respectively. These two entities display somewhat different imaging features, which are important to recognize.

Rheumatoid arthritis is an autoimmune disease which causes the human body’s own immune system to attack and often destroy the lining of the joints. Although it commonly affects the small joints of the hands and feet, rheumatoid arthritis, or RA, can affect any joint in the human body. The neck, or cervical spine, can be affected more often than the lower back if rheumatoid arthritis affects the joints in the spine.
Dr. Alex Jimenez D.C., C.C.S.T.
Rheumatoid Arthritis
Involvement in RA is usually located in the cervical spine where erosive changes are predominantly seen in the atlanto-axial region. Inflamed and thickened synovium (pannus) can occur around the odontoid process (dens) and cause bone erosion and destruction of surrounding ligaments, most seriously if the posterior transverse ligament is involved. Laxity or rupture of the transverse ligament causes instability with a potential risk of spinal cord injury. Cervical RA involvement is a progressive, serious condition with reduced lifetime expectancy [1], and its diagnosis is therefore important [2, 3].

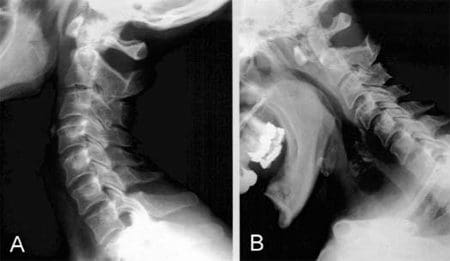
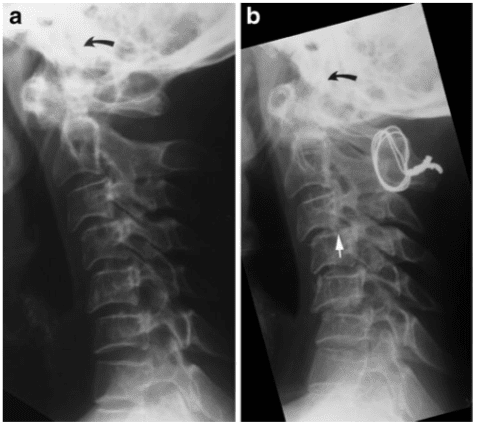
Radiography of the cervical spine is mandatory in RA patients with neck pain [3]. It should always include a lateral view in a flexed position compared with a neutral position in addition to special views of the dens area to detect any lesions and/or instability (Fig. 1). A supplementary lateral view during extension can be useful to assess reducibility of atlanto-axial subluxation possibly limited by pannus tissue between the anterior arc of the atlas and dens.
Anterior atlanto-axial subluxation is the most frequent form of RA instability in the occipito-atlanto-axial region, but lateral, rotatory and vertical subluxation can also occur. The definition of the different forms of instability by radiography is as follows [3].
Anterior atlanto-axial subluxation. Distance between the posterior aspect of the anterior arc of the atlas and the anterior aspect of the dens exceeding 3 mm in a neutral position and/or during flexion (Fig. 1). It may cause stenosis of the atlanto-axial canal presenting as a posterior atlanto-dental interval<14 mm (Fig. 1).
Lateral and rotatory atlanto-axial subluxation. Displacement of the lateral masses of the atlas more than 2 mm in relation to that of the axis and asymmetry of the lateral masses relative to the dens, respectively (Fig. 2). Rotatory and lateral subluxation is diagnosed on open-mouth anterior-posterior (AP) radiographs. Anterior subluxation often coexists because of the close anatomical relation between the atlas and the axis.
Posterior atlanto-axial subluxation. The anterior arc of the atlas moves over the odontoid process. This is rarely seen, but may coexist with fracture of the dens.
Vertical atlanto-axial subluxation is also referred to as atlanto-axial impaction, basilar invagination or cranial setting, and is defined as migration of the odontoid tip proximal to McRae’s line corresponding to the occipital foramen. This line can be difficult to define on radiographs, and vertical subluxation has therefore also been defined by several other methods. Migration of the tip of the odontoid process >4.5 mm above McGregor’s line (between the postero-superior aspect of the hard palate and the most caudal point of the occipital curve) indicates vertical subluxation (Fig. 3).
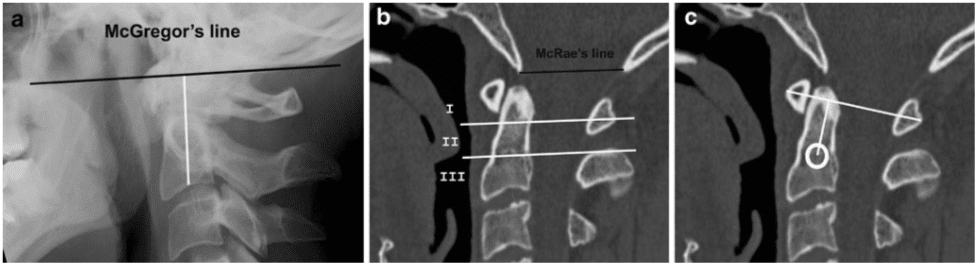
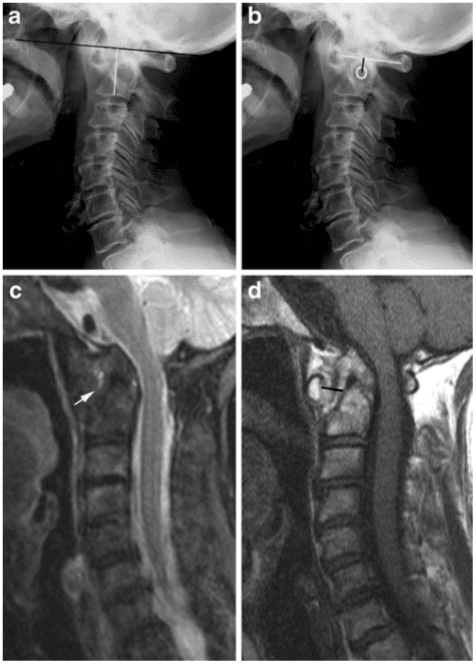
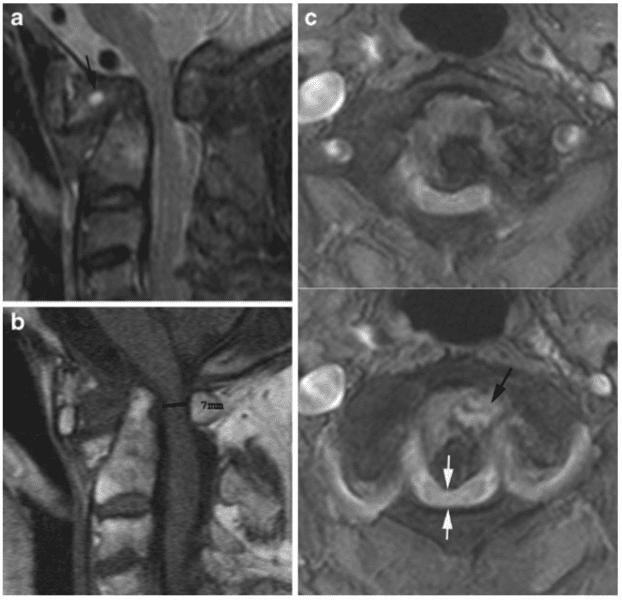
The occurrence of dens erosion can, however, make this measurement difficult to obtain. The Redlund-Johnell method is therefore based on the minimum distance between McGregor’s line and the midpoint of the inferior margin of the body of the axis on a lateral radiograph in a neutral position (Fig. 3) [4]. Visualisation of the palate may not always be obtained. Methods without dens and/or the palate as landmarks have therefore been introduced [4]. The method described by Clark et al. (described in [4]) includes assessment of the location of the atlas by dividing the axis into three equal portions on a lateral radiograph. Location of the anterior arc of the atlas in level with the middle or caudal third of the axis indicates vertical subluxation (Fig. 3). Ranawat et al. have proposed using the distance between the centre of the second cervical pedicle and the transverse axis of the atlas at the odontoid process (Fig. 3) [4]. To obtain the diagnosis of vertical subluxation a combination of the Redlund-Johnell, Clark and Ranawat methods has been recommended (described in [4]). If any of these methods suggests vertical subluxation MRI should be performed to visualize the spinal cord (Fig. 4). Using this combination of methods vertical subluxation will be missed in only 6% of patients [4]. It is mandatory to diagnose vertical subluxation; this can be fatal because of the proximity of the dens to the medulla oblongata and the proximal portion of the spinal cord. Risk of cord compression/injury occurs, especially in patients with flexion instability accompanied by erosive changes in the atlanto- axial and/or atlanto-occipital joints, causing the vertical subluxation with protrusion of the dens into the occipital foramen (Figs. 4, 5).
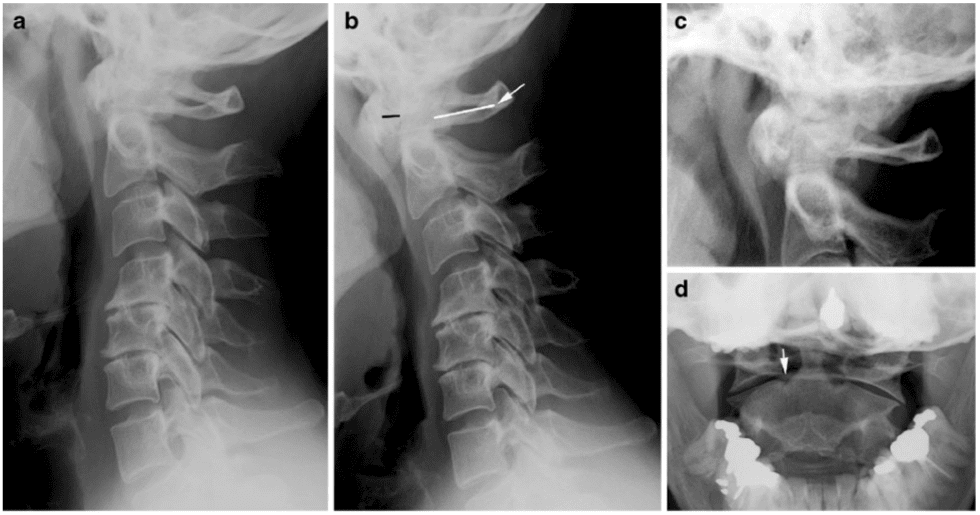
Subaxial RA changes also occur in the form of arthritis of the apophyseal and/or uncovertebral joints, appearing as narrowing and superficial erosions by radiography. It can cause instability in the C2-Th1 region, which is mainly seen in patients with severe chronic peripheral arthritis. Anterior subluxation is far more frequent than posterior subluxation. It is defined as at least 3 mm forward slippage of a vertebra relative to the underlying vertebra by radiography including a flexion view (Fig. 6). Changes are particularly characteristic at the C3–4 and C4–5 level, but multiple levels may be involved, producing a typical “stepladder” appearance on lateral radiographs. The condition is serious if the subaxial sagittal spinal canal diameter is <14 mm, implying a possibility of spinal cord compression [2]. The instability may progress over time, especially if the C1–C2 region is stabilized surgically (Fig. 6) [5].
Discitis-like changes and spinous process erosion may also be detected by radiography in RA, but are relatively rare, whereas concomitant degenerative changes occur occasionally (Fig. 1).
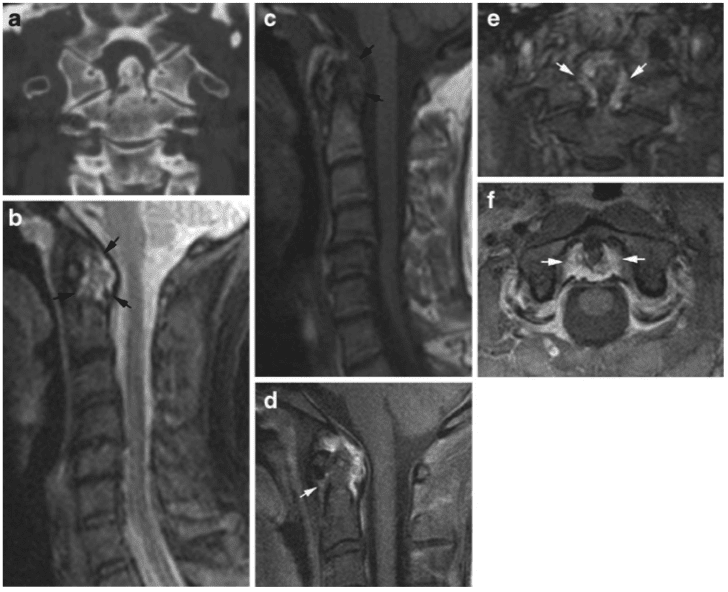
Cross-sectional imaging in the form of CT and MRI eliminates overprojecting structures and can improve the detection of RA changes. Osseous changes (erosions, etc.) can be clearly delineated by CT [6]. Additionally, MRI visualizes soft tissue structures (pannus; spinal cord, etc.), signs of disease activity and sequelae of inflammation in the form of fibrous pannus. These advantages of CT and MRI in patients with atlanto-axial involvement are illustrated in Figs. 7 and 8, including the possibility of detecting signs of arthritis by MRI before the occurrence of erosive changes (Fig. 8) [3].
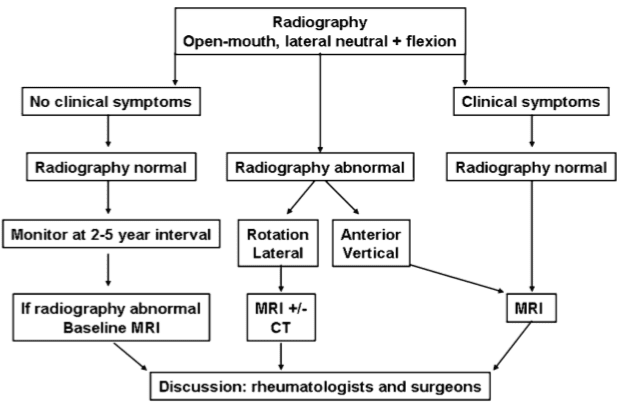
A diagnostic strategy according to Younes et al. [3] is recommended (Fig. 9). This includes an indication for radiography in all RA patients with disease duration >2 years as cervical involvement may occur in over 70% of patients and has been reported to be asymptomatic in 17% of RA patients. It is recommended to monitor patients with manifest peripheral erosions accompanied by RF (rheumatoid factor) and antiCCP (antibodies to cyclic citrullinated peptide) positivity every second year and patients with few peripheral erosions and RF negativity at 5-year intervals. MRI is indicated in patients with neurological deficit, radiographic instability, vertical subluxation and subaxial stenosis [2, 3]. Visualisation of the spinal cord is especially important to detect cord injury or risk of injury. MRI should therefore always be performed in RA patients with neck pain and/or neurological symptoms [3, 7].
Seronegative Spondyloarthritides
According to European classification criteria [8, 9], SpA is divided into: (1) ankylosing spondylitis (AS), (2) psoriatic arthritis, (3) reactive arthritis, (4) arthritis associated with inflammatory bowel disorders (enteropathic arthritis) and (5) undifferentiated SpA. Inflammatory changes at the sacroiliac joints always occur in AS and are part of most other forms of SpA. Spinal changes are also a feature of SpA, especially in the late stages of AS.
Ankylosing Spondylitis
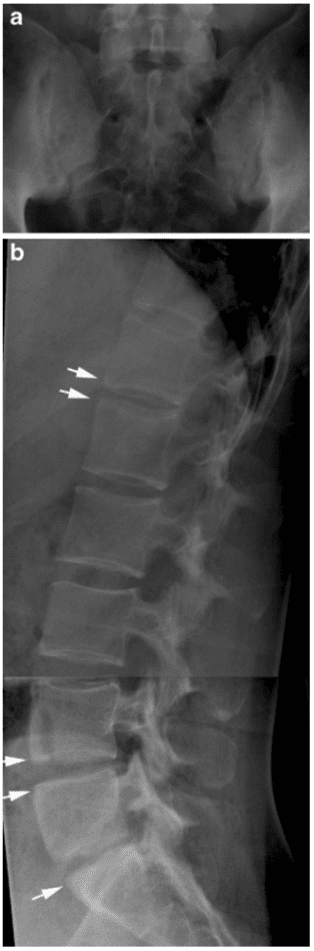
Ankylosing spondylitis is the most frequent and usually the most disabling form of SpA. It has a genetic predisposition in the form of a frequent association with the human leukocyte antigen (HLA) B27 [10]. AS often starts in early adulthood and has a chronic progressive course. It is therefore important to diagnose this disorder. According to the modified New York Criteria [11], the diagnosis of definite AS requires the following: manifest sacroiliitis by radiography (grade ≥2 bilateral or unilateral grade 3–4 sacroiliitis; Fig. 10) and at least one of the following clinical criteria: (1) low back pain and stiffness for more than 3 months improving with activity, (2) limited movement of the lumbar spine and (3) reduced chest expansion. These criteria are still used in the diagnosis of AS despite the increasing use of MRI to detect the disease early. It is therefore important to know both the characteristic radiographic features and the MR features of AS.
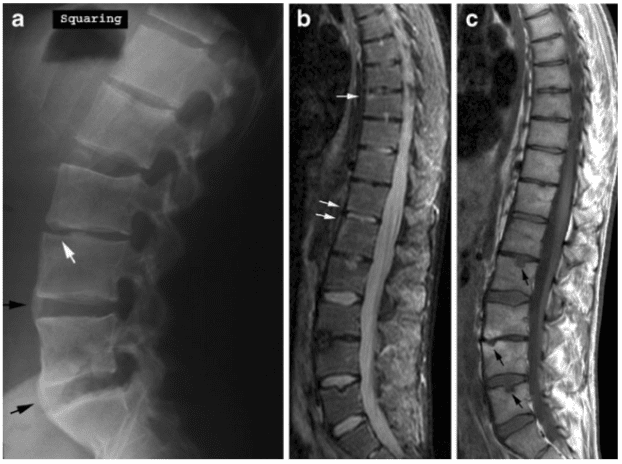
Early radiographic spinal changes encompass erosion of vertebral corners (Romanus lesions) causing vertebral squaring and eliciting reactive sclerosis appearing as condensation of vertebral corners (shiny corners; Fig. 10). These changes are caused by inflammation at the insertion of the annulus fibrosus (enthesitis) at vertebral corners provoking reactive bone formation [12]. Later on slim ossifications appear in the annulus fibrosus (syndesmo- phytes) (Fig. 11) [13]. With disease progression the spine gradually fuses because of syndesmophytes crossing the intervertebral spaces in addition to fusion of apophyseal joints, resulting in complete spinal fusion (bamboo spine; Fig. 12). In advanced disease the supra- and interspinous ligaments may ossify and be visible on frontal radiographs as a slim ossified streak (Fig. 12). The occurrence of a single central radiodense streak has, the “dagger sign”. When the ligamentous ossification occurs together with ossification of apophyseal joint capsules, there are three vertical radiodense lines on frontal radiography (trolley-track sign).
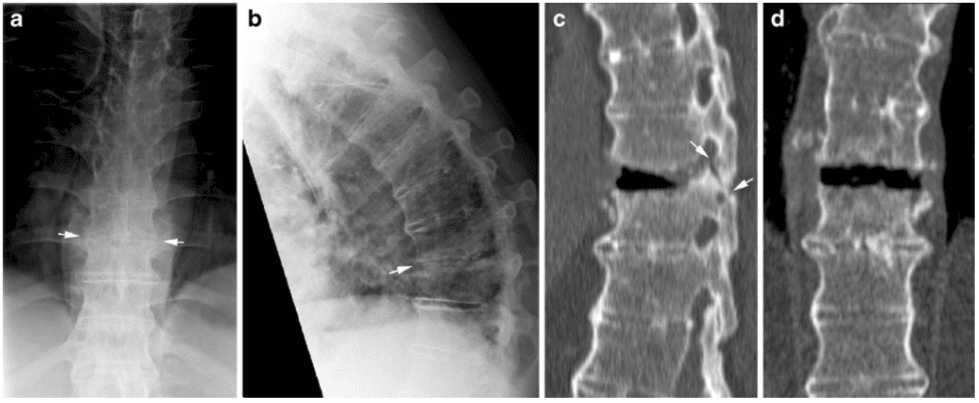
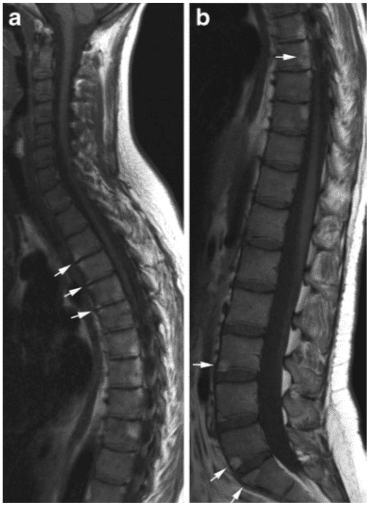
Erosive changes within intervertebral spaces (Andersson lesions) have been detected by radiography in approximately 5% of patients with AS [14], but more frequently by MRI (Fig. 11) [15].
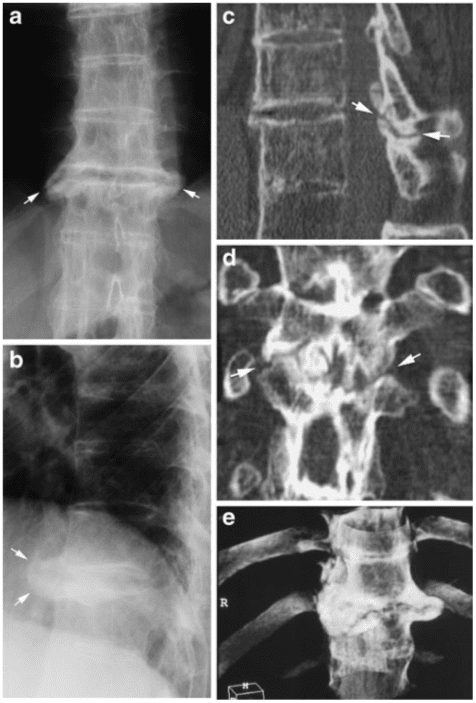
Persistent movement at single intervertebral spaces may occur in an otherwise ankylosed spine, sometimes caused by non-diagnosed fractures. This can result in pseudo- arthrosis-like changes with the formation of surrounding reactive osteophytes due to excessive mechanical load at single movable intervertebral spaces [14]. The diagnosis of such changes may require a CT examination to obtain adequate visualization (Fig. 13).
One of the life-threatening complications of AS is spinal fracture. Non-fatal fractures have been reported to occur in up to 6% of AS patients, especially in patients with long disease duration [16]. Fractures may occur after minor trauma because of the spinal stiffness and frequently accompanying osteoporosis. Fractures often occur at intervertebral spaces, but usually involve the ankylosed posterior structures and are thereby unstable (Fig. 14). Obvious fractures can visualize by radiography, but fractures may be obscured. It is therefore mandatory to supplement a negative radiography with CT if fracture is suspected (in the case of trauma history or a change in spinal symptoms). The occurrence of cervico-thoracic fractures may cause spinal cord injury and be lethal even following minor trauma [17].
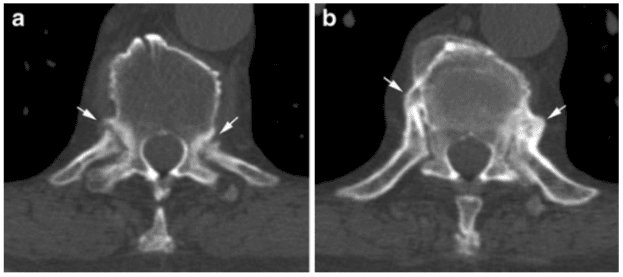
Cross-sectional CT or MR imaging can be advantageous in the diagnosis of AS changes. CT providing a clear delineation of osseous structures is the preferred technique for visualizing pseudo-arthrosis and detecting fractures (Figs. 13, 14). CT is superior to MRI in detecting minor osseous lesions such as erosion and ankylosis of the apophyseal, costo-vertebral and costo-transversal joints (Fig. 15). MRI can visualize signs of active inflammation in the form of bone marrow and soft tissue oedema and/or contrast enhancement. It has therefore gained a central role in the evaluation of disease activity [15]. MRI can, however, also detect sequelae of inflammation consisting of fatty deposition in the bone marrow and chronic structural changes such as erosion and fusion of vertebral bodies [15].
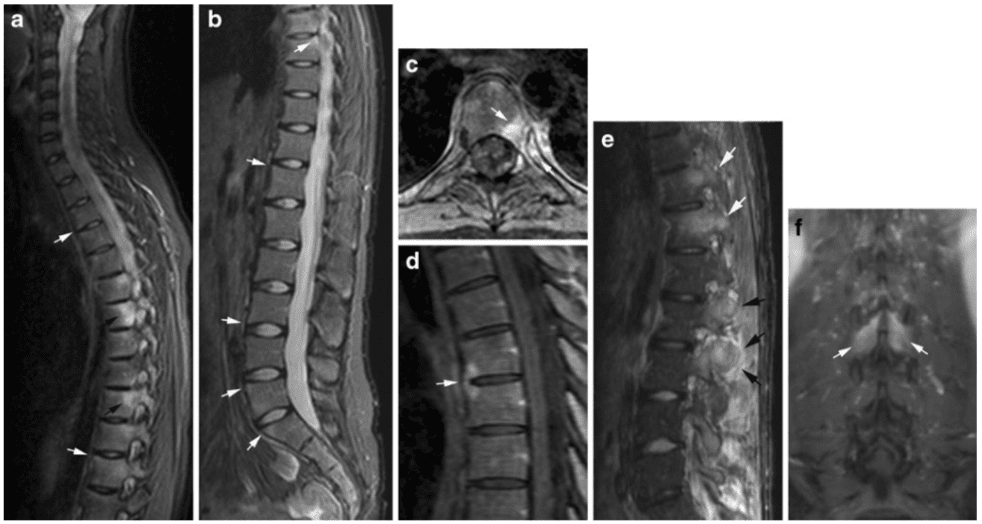
Characteristic MR findings early in the disease are activity changes mainly consisting of oedema at vertebral corners and/or costo-vertebral joints (Fig. 16) [13]. The inflammatory changes at vertebral corners are characteristic of AS. Based on the occurrence of severe or multiple (≥3) lesions in young patients, AS changes can be distinguished from degenerative changes with a high reliability [18].
During the disease course signs of activity can also occur at syndesmophytes, apophyseal joints and interspinous ligaments (Fig. 16). Detection of inflammation at apophyseal joints by MRI, however, demands pronounced involvement histopathologically [19]. The inflammation at vertebral corners is the most valid feature and has been observed related to the development of syndesmophytes by radiography [12], establishing a link between signs of disease activity and chronic structural changes.
Chronic AS changes detectable by MRI mainly consist of fatty marrow deposition at vertebral corners (Fig. 17), erosion (Fig. 11) and vertebral fusion in advanced disease (Fig. 12). Fatty marrow deposition seems to be an a sign of chronicity being significantly correlated with radiographic changes, in particular, vertebral squaring [15]. Erosions are more frequently detected by MRI than by radiography (Fig. 11) [15] and can present with signs of active inflammation and/or surrounding fatty marrow deposition compatible with sequels of osseous inflammation. Syndesmophytes, however, may not always be visible by MRI because they may be difficult to distinguish from fibrous tissue unless there is concomitant active inflammation or fatty deposition (Figs. 11, 16) [15, 20].
The possibility of visualizing disease activity by MRI has increased its use to monitor AS, especially during anti-TNF (anti-tumour necrosis factor) therapy [21, 22]. Several studies have shown that MR changes are frequent in the thoracic spine (Fig. 16) [15, 23]. It is therefore important to examine the entire spine using sagittal STIR or T2 fat-saturated (FS) and T1-weighted sequences. Supplementary axial slices can be necessary for visualising involvement of apophyseal, costo-vertebral and costo-transversal joints (Fig. 16) [24, 25]. Post-contrast T1FS sequences can sometimes be advantageous as they provide better anatomical delineation [26]. Additionally, dynamic contrast-enhanced MRI may be superior to static MRI in monitoring disease activity during anti-TNF therapy [27]. Whole-body MRI gives the possibility of detecting involvement in other areas without losing important information about spinal and sacroiliac joint involvement [28, 29].
Other Forms of SpA
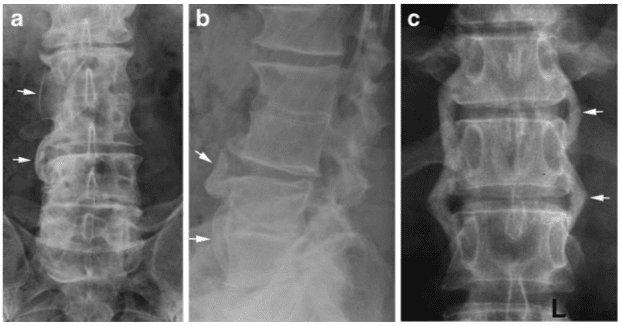
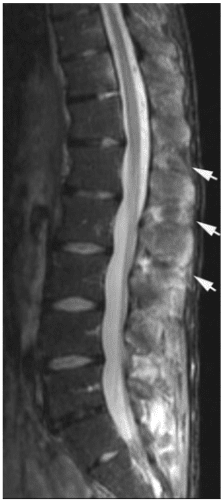
Radiographic changes in reactive and psoriatic arthritis are often characterized by voluminous non-marginal syndesmophytes (parasyndesmophytes) or coalescing ossification of the paravertebral ligaments in addition to asymmetrical sacroiliitis (Fig. 18) [30].
Reactive arthritis is self-limiting in most patients. However, in patients with chronic reactive arthritis and HLA B27 the axial changes may progress to changes somewhat similar to those seen in AS and can then be regarded as AS elicited by infection [10].
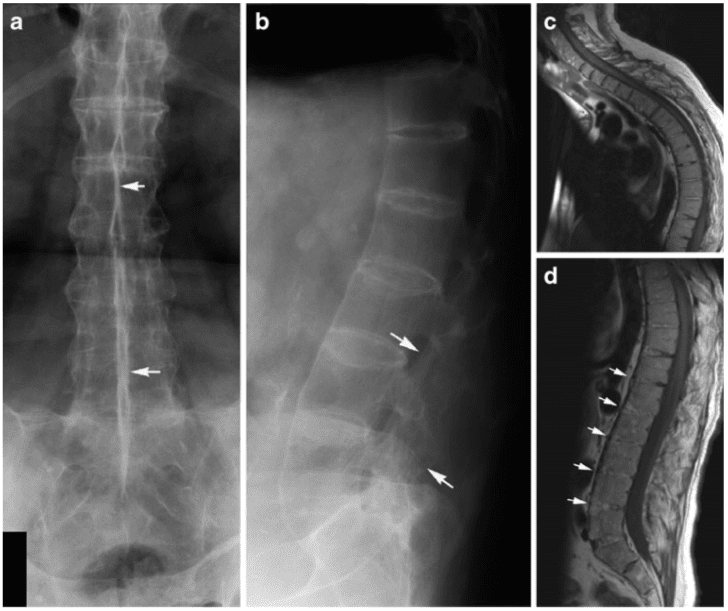
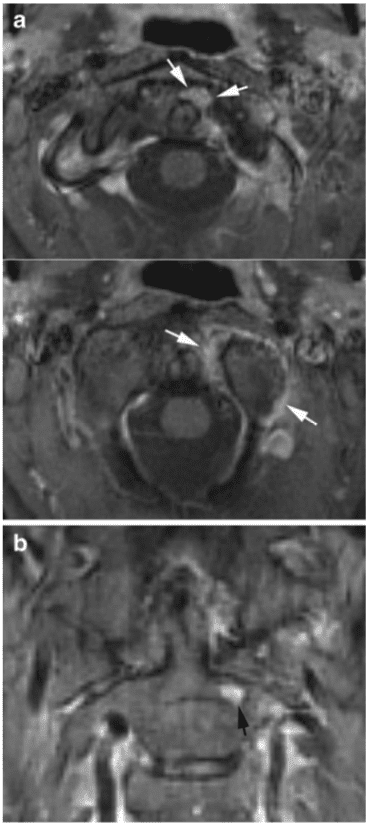
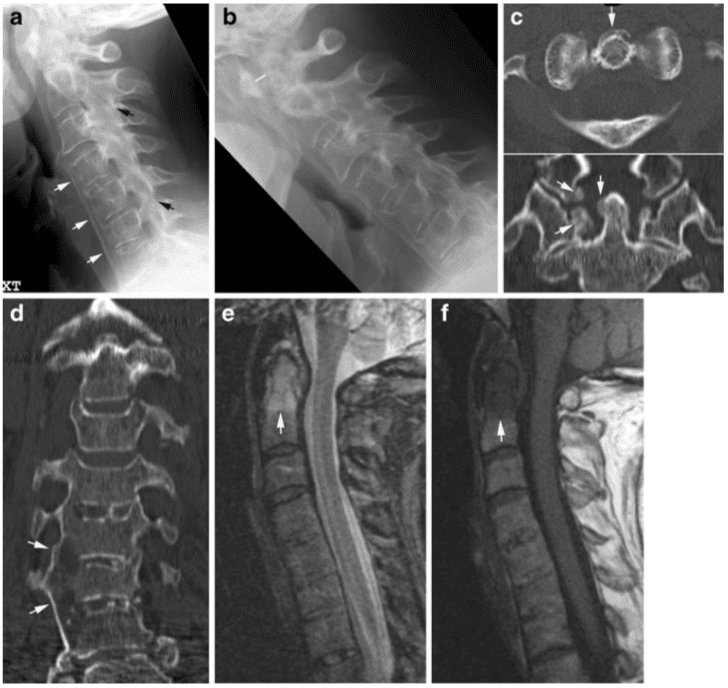
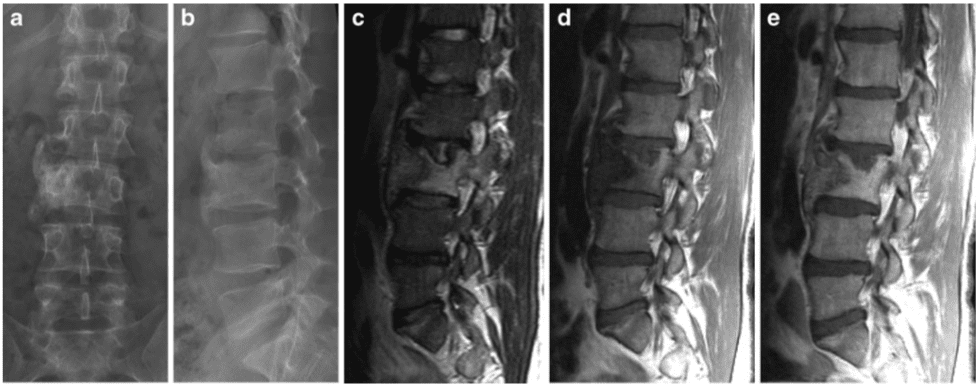
Axial psoriatic arthritis (PsA) occurs in approximately 50% of patients with peripheral PsA [31]. It differs radiographically from AS by the voluminous paravertebral ossifications and the occurrence of spinal changes without concomitant sacroiliitis in 10% of patients [32]. Axial PsA may be clinically silent [33], and involvement of the cervical spine is frequent (atlanto-axial or apophyseal joint changes). The cervical recognize may include atlanto-axial instability as seen in RA (Fig. 19), but the pathogenesis and thereby imaging findings are different. In PsA radiography and CT usually visualize new bone formation in the region of the dens. This is elicited by osseous inflammation (osteitis) and/or inflammation at ligament/ tendon attachments (enthesitis) detectable by MRI (Fig. 19). Osteitis is often a feature of spinal PsA and can occur together with paravertebral ossification/para- syndesmophytes and erosion of vertebral plates (Fig. 20). , and illustrated MR findings in PsA are based on personal observations and seem to reflect the radiographic changes encompassing a mixture of osteitis, enthesitis and erosion. Unfortunately, there is a lack of systematic description of spinal changes in PsA by MRI. Some of the patients described under the term SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome may have PsA. SAPHO is a collective term often used for inflammatory disorders primarily presenting with osseous hyperostosis and sclerosis, and they are frequently associated with skin disorders. The most commonly affected site in SAPHO is the anterior chest followed by the spine [34]. The PsA changes shown in Fig. 20 are characterized by hyperostosis and sclerosis, both main features of SAPHO. However, this patient did not have anterior chest involvement.
In patients with enteropathic arthritis associated with Crohn’s disease or ulcerative colitis, the spine is often osteoporotic with various accompanying SpA features by radiography, mostly AS-like changes. However, by MRI there may be more pronounced inflammation in the posterior ligaments than seen in the other forms of SpA (Fig. 21).

Rheumatoid arthritis of the spine can cause neck pain, back pain, and/or radiating pain in the upper and lower extremities. In severe cases, RA can also lead to the degeneration of the spine, resulting in the compression or impingement of the spinal cord and/or the spinal nerve roots. As a chiropractor, we offer diagnostic imaging to help determine a patient’s health issue, in order to develop the best treatment program.
Dr. Alex Jimenez D.C., C.C.S.T.
Conclusion
Radiography is still valuable in the diagnosis of spinal inflammatory disorders. It is necessary for visualizing instability and is superior to MRI for detecting syndesmophytes. However, MRI and CT can detect signs of spinal involvement before they can be visualized by radiography. MRI adds information about potential involvement of the spinal cord and nervous roots in addition to signs of disease activity and chronic changes such as fibrous pannus in RA and fatty marrow deposition, erosion and vertebral fusion in SpA. MRI is therefore widely used to monitor inflammatory spinal diseases, especially during anti-TNF therapy.
Computed tomography is particularly valuable in the detection of fracture and minor osseous lesions as well as in the evaluation of pseudo-arthrosis. In conclusion, rheumatoid arthritis most commonly affects the structure and function of your hands, wrists, elbows, hips, knees, ankles and feet, however, people with this chronic inflammatory disease can experience back pain. Imaging the spine in arthritis is fundamental to determine treatment. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez

Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.

EXTRA IMPORTANT TOPIC: Sciatica Pain Chiropractic Therapy
Post Disclaimer
Professional Scope of Practice *
The information herein on "Imaging the Spine in Arthritis: a Pictorial Review" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Our information scope is limited to Chiropractic, musculoskeletal, physical medicines, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somatovisceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and/or functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and directly or indirectly support our clinical scope of practice.*
Our office has reasonably attempted to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez, DC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, RN*, CCST, IFMCP*, CIFM*, ATN*
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807, New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Florida
Florida License RN License # RN9617241 (Control No. 3558029)
License Compact Status: Multi-State License: Authorized to Practice in 40 States*
Presently Matriculated: ICHS: MSN* FNP (Family Nurse Practitioner Program)
Dr. Alex Jimenez DC, MSACP, RN* CIFM*, IFMCP*, ATN*, CCST
My Digital Business Card